

The effect of postoperative stroke and myocardial infarction on long-term survival after carotid revascularization
- PMID: 23402875
- PMCID: PMC3930446
- DOI: 10.1016/j.jvs.2012.11.118
The effect of postoperative stroke and myocardial infarction on long-term survival after carotid revascularization
Abstract
Introduction: The largest randomized controlled trial that compared the efficacy of carotid endarterectomy (CEA) with carotid artery stenting (CAS) showed equivalent outcomes for the composite end point of postoperative stroke, myocardial infarction (MI), or death. However, CAS had a higher risk of postoperative stroke, and CEA had a higher risk of MI. We hypothesize that there is a differential association of postoperative stroke, compared with that of postoperative MI, with reduced long-term survival after carotid revascularization when compared with neither complication.
Methods: The Vascular Study Group of New England database was used to identify all CEA and CAS procedures performed between 2003 and 2011. Patients were stratified according to whether they experienced an in-hospital postoperative stroke (minor or major), MI (troponin elevation, electrocardiographic changes, or clinical symptoms), or neither. Primary study end point was survival during the first year and the first 5 years postoperatively. Multivariable Cox proportional hazards models compared the magnitude of association of stroke and MI on survival.
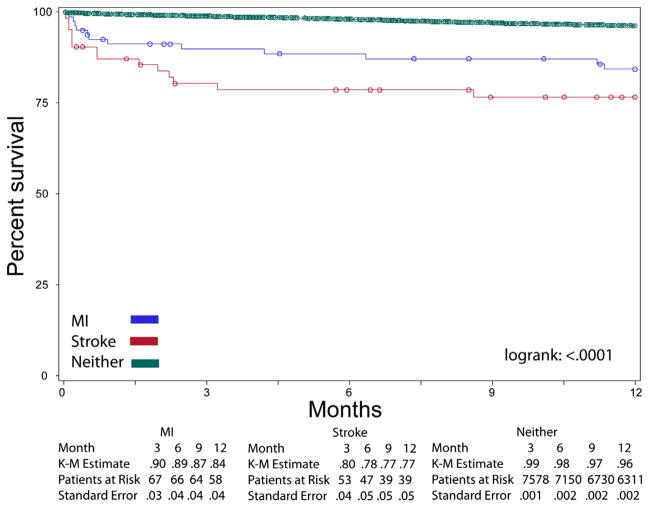
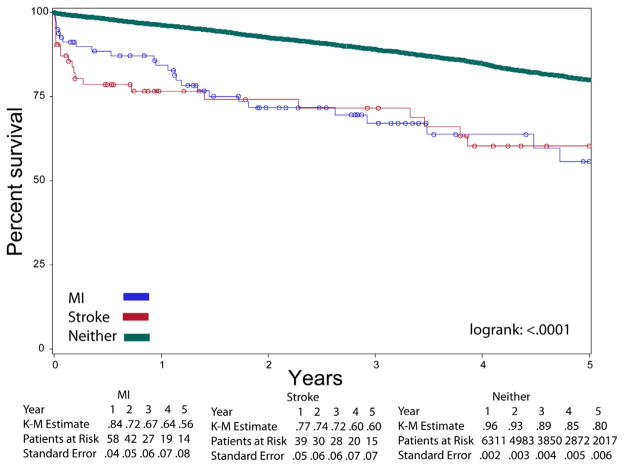
Results: Of 8315 patients, 81 (0.97%) experienced postoperative MI, and 63 (0.76%) experienced stroke. During the first year after operation, survival significantly differed among the three groups: neither, 96%; MI, 84%; stroke, 77% (log-rank P < .0001). After adjusting for confounders, survival after postoperative stroke (hazard ratio [HR], 6.6; 95% confidence interval [CI], 3.7-12; P < .0001) was nearly twofold less than that after postoperative MI (HR, 3.6; 95% CI, 2-6.8; P < .0001). During the first 5 years postoperatively, multivariable modeling showed postoperative stroke and postoperative MI remained independent predictors of decreased survival, but the magnitude of association was similar (HR, 2.7; 95% CI, 1.7-4.3 [P < .0001] vs HR, 2.8; 95% CI, 1.8-4.3 [P < .0001]).
Conclusions: During the first year after operation, postoperative stroke conferred a twofold lower survival than that after postoperative MI. By 5 years after operation, these survival curves converged, and the survival disadvantage associated with stroke became similar to that of MI. These data suggest that different postoperative complications after carotid revascularization have different implications for patients, with decreased short-term survival in patients experiencing a postoperative stroke. These findings help to inform our interpretation of studies that have used a composite end point in order to evaluate the comparative effectiveness of revascularization strategies.
Copyright © 2013 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
References
-
- Mas JL, Chatellier G, Beyssen B, Branchereau A, Moulin T, Becquemin JP, et al. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660–71. - PubMed
-
- Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Protected carotidartery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351:1493–501. - PubMed
-
- Eckstein HH, Ringleb P, Allenberg JR, Berger J, Fraedrich G, Hacke W, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol. 2008;7:893–902. - PubMed
-
- Ederle J, Dobson J, Featherstone RL, Bonati LH, van der Worp HB, de Borst GJ, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet. 2010;375:985–97. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
