

Gd-EOB-DTPA-enhanced MRI for the assessment of liver function and volume in liver cirrhosis
- PMID: 23403453
- PMCID: PMC3664988
- DOI: 10.1259/bjr.20120653
Gd-EOB-DTPA-enhanced MRI for the assessment of liver function and volume in liver cirrhosis
Abstract
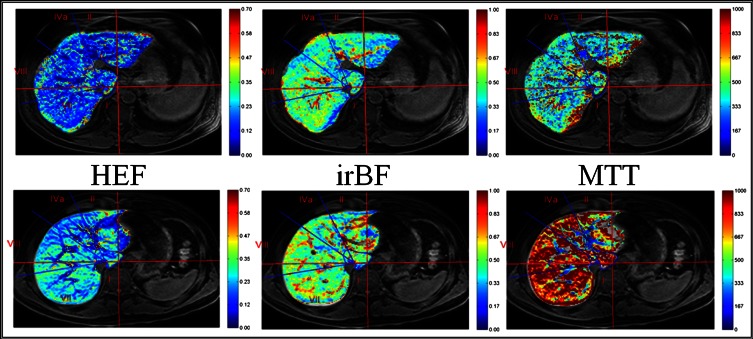
Objective: The aims of this study were to use dynamic hepatocyte-specific contrast-enhanced MRI to evaluate liver volume and function in liver cirrhosis, correlate the results with standard scoring models and explore the inhomogeneous distribution of liver function in cirrhotic livers.
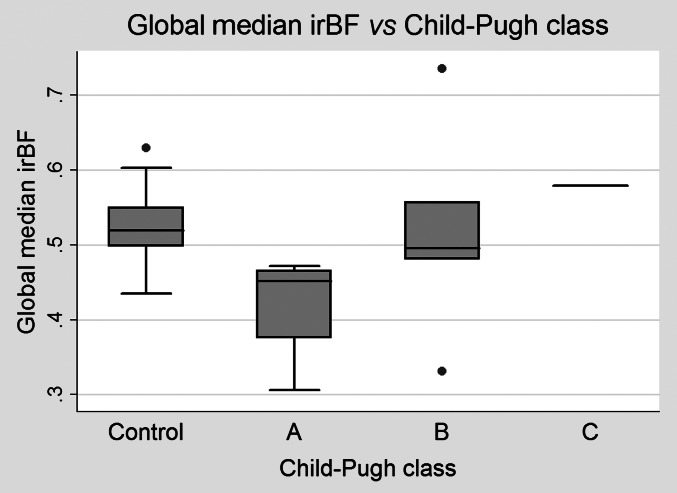
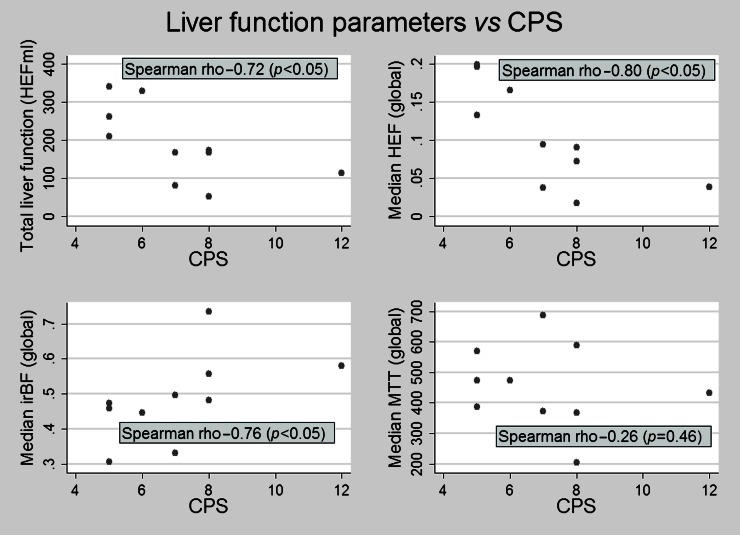
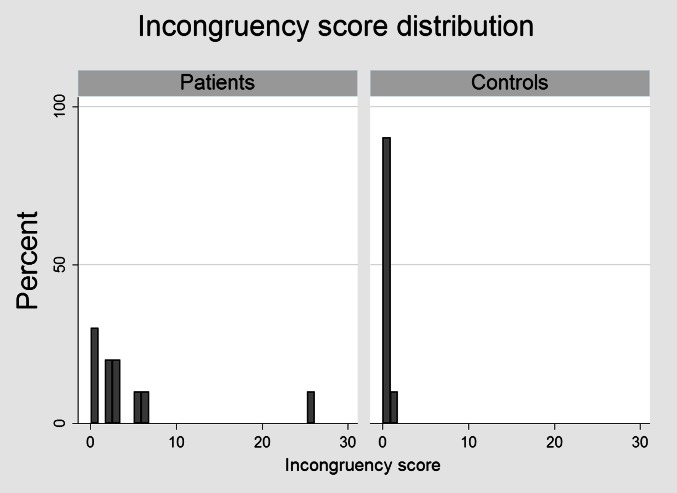
Methods: 10 patients with liver cirrhosis and 20 healthy volunteers, serving as controls, were included. Hepatic extraction fraction (HEF), input relative blood flow and mean transit time were calculated on a voxel-by-voxel basis using deconvolutional analysis. Segmental and total liver volumes as well as segmental and total hepatic extraction capacity, expressed in HEFml, were calculated. An incongruence score (IS) was constructed to reflect the uneven distribution of liver function. The Mann-Whitney U-test was used for group comparison of the quantitative liver function parameters, liver volumes and ISs. Correlations between liver function parameters and clinical scores were assessed using Spearman rank correlation.
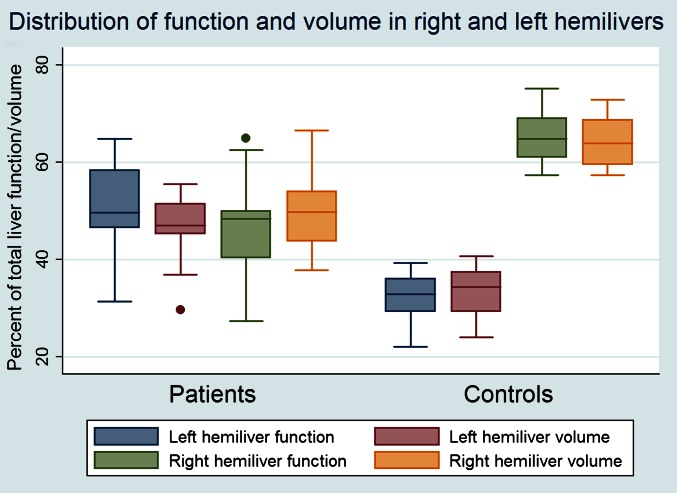
Results: Patients had larger parenchymal liver volume, lower hepatocyte function and more inhomogeneous distribution of function compared with healthy controls.
Conclusion: The study demonstrates the non-homogeneous nature of liver cirrhosis and underlines the necessity of a liver function test able to compensate for the heterogeneous distribution of liver function in patients with diseased liver parenchyma.
Advances in knowledge: The study describes a new way to quantitatively assess the hepatic uptake of gadoxetate or gadolinium ethoxybenzyl diethylenetriaminepentaacetic acid in the liver as a whole as well as on a segmental level.
Figures
References
-
- Sakamoto S, Uemoto S, Uryuhara K, Kim Id, Kiuchi T, Egawa H, et al. Graft size assessment and analysis of donors for living donor liver transplantation using right lobe. Transplantation 2001;71:1407–13 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
