

Effect of a single session of muscle-biased therapy on pain sensitivity: a systematic review and meta-analysis of randomized controlled trials
- PMID: 23403507
- PMCID: PMC3569047
- DOI: 10.2147/JPR.S37272
Effect of a single session of muscle-biased therapy on pain sensitivity: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Muscle-biased therapies (MBT) are commonly used to treat pain, yet several reviews suggest evidence for the clinical effectiveness of these therapies is lacking. Inadequate treatment parameters have been suggested to account for inconsistent effects across studies. Pain sensitivity may serve as an intermediate physiologic endpoint helping to establish optimal MBT treatment parameters. The purpose of this review was to summarize the current literature investigating the short-term effect of a single dose of MBT on pain sensitivity in both healthy and clinical populations, with particular attention to specific MBT parameters of intensity and duration.
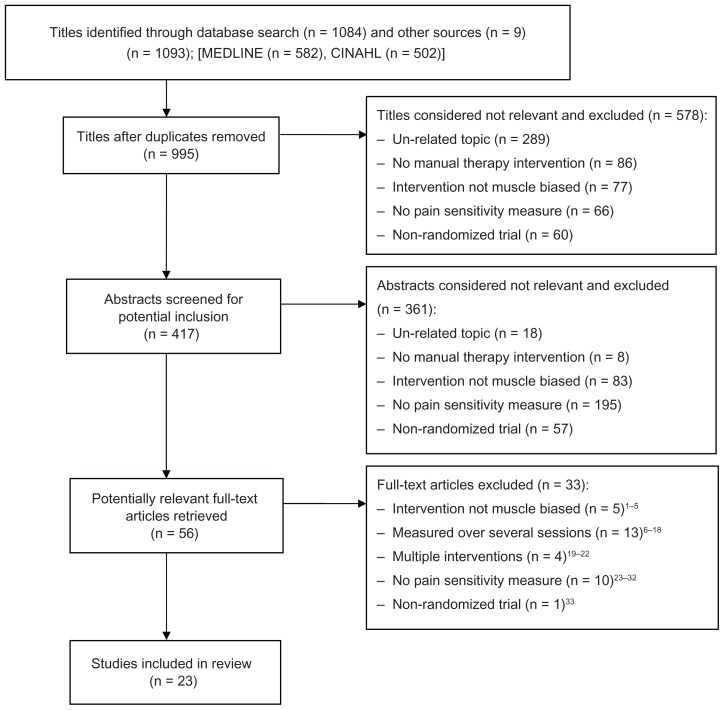
Methods: A systematic search for articles meeting our prespecified criteria was conducted using Cumulative Index to Nursing and Allied Health Literature (CINAHL) and MEDLINE from the inception of each database until July 2012, in accordance with guidelines from the Preferred Reporting Items for Systematic reviews and Meta-Analysis. Relevant characteristics from studies included type, intensity, and duration of MBT and whether short-term changes in pain sensitivity and clinical pain were noted with MBT application. Study results were pooled using a random-effects model to estimate the overall effect size of a single dose of MBT on pain sensitivity as well as the effect of MBT, dependent on comparison group and population type.
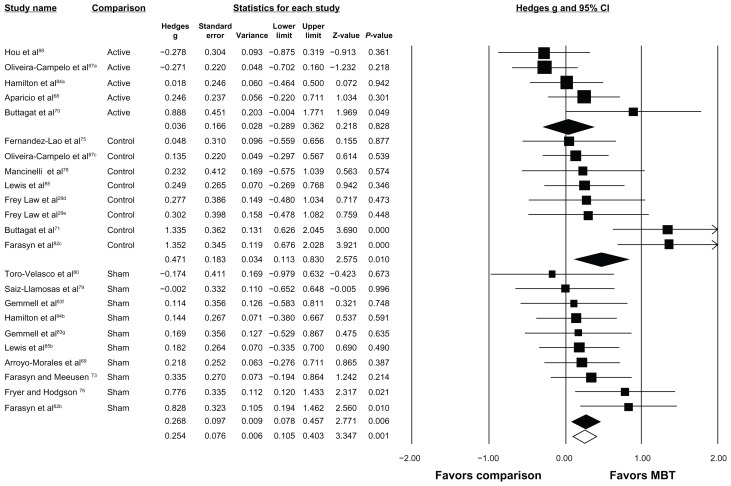
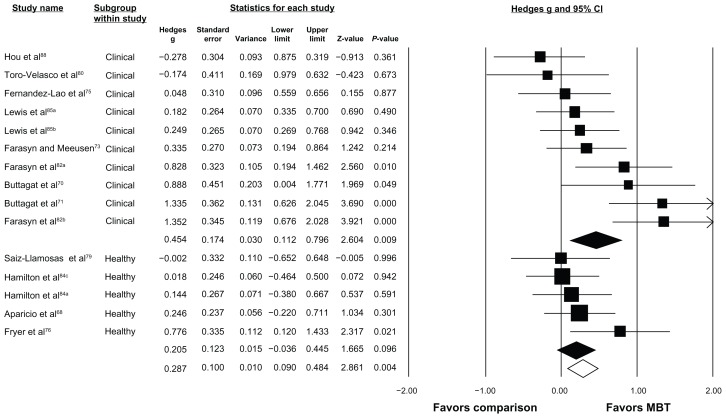
Results: Reports from 24 randomized controlled trials (23 articles) were included, representing 36 MBT treatment arms and 29 comparative groups, where 10 groups received active agents, 11 received sham/inert treatments, and eight received no treatment. MBT demonstrated a favorable and consistent ability to modulate pain sensitivity. Short-term modulation of pain sensitivity was associated with short-term beneficial effects on clinical pain. Intensity of MBT, but not duration, was linked with change in pain sensitivity. A meta-analysis was conducted on 17 studies that assessed the effect of MBT on pressure pain thresholds. The results suggest that MBT had a favorable effect on pressure pain thresholds when compared with no-treatment and sham/inert groups, and effects comparable with those of other active treatments.
Conclusion: The evidence supports the use of pain sensitivity measures by future research to help elucidate optimal therapeutic parameters for MBT as an intermediate physiologic marker.
Keywords: muscle-biased therapy; pain sensitivity; pressure pain threshold.
Figures
References
-
- Lund I. Massage as a pain relieving method. Physiotherapy. 2000;86:638–639.
-
- Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1–23. - PubMed
-
- Bercovitz A, Sengupta M, Jones A, Harris-Kojetin L. Complementary and Alternative Therapies in Hospice: The National Home and Hospice Care Survey: United States, 2007. Hyattsville, MD: National Center for Health Statistics; [Accessed November 13, 2012]. Available from: http://www.cdc.gov/nchs/data/nhsr/nhsr033.pdf. - PubMed
-
- Kanodia AK, Legedza AT, Davis RB, Eisenberg DM, Phillips RS. Perceived benefit of complementary and alternative medicine (CAM) for back pain: a national survey. J Am Board Fam Med. 2010;23:354–362. - PubMed
-
- Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;18:1–14. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
