

Delirium and Long-term Cognitive Trajectory Among Persons With Dementia
- PMID: 23403619
- PMCID: PMC3740440
- DOI: 10.1001/archinternmed.2012.3203
Delirium and Long-term Cognitive Trajectory Among Persons With Dementia
Abstract
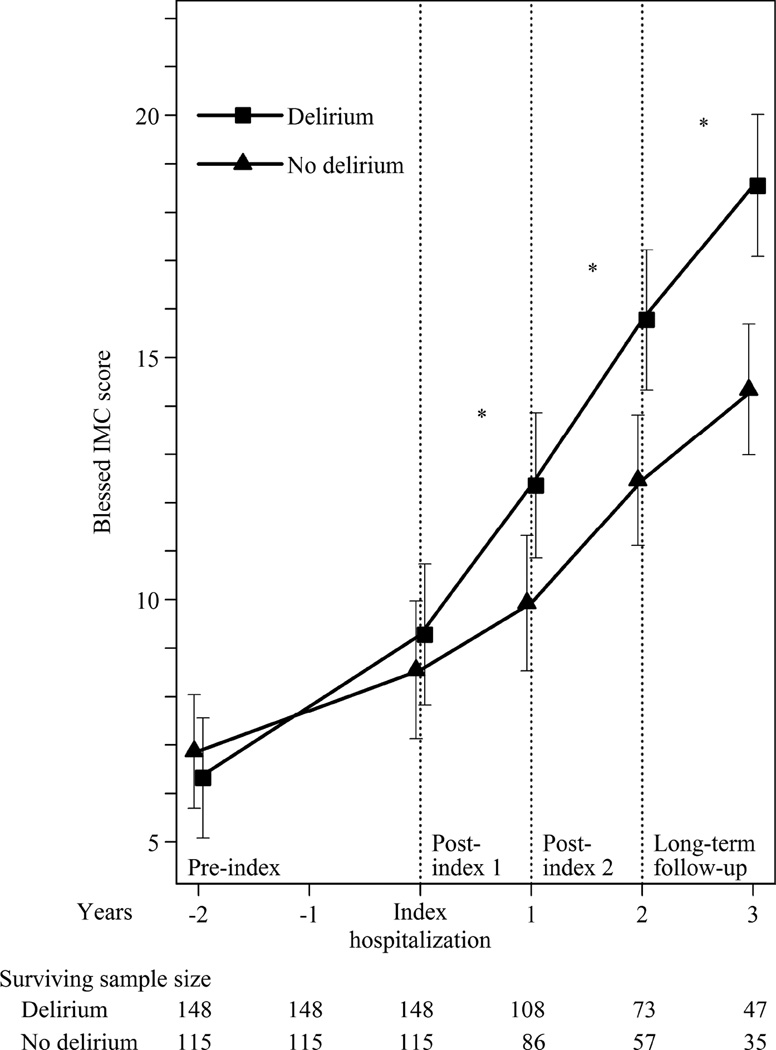
BACKGROUND Delirium is characterized by acute cognitive impairment. We examined the association of delirium with long-term cognitive trajectories in older adults with Alzheimer disease (AD). METHODS We evaluated prospectively collected data from a nested cohort of hospitalized patients with AD (n = 263) in the Massachusetts Alzheimer Disease Research Center patient registry between January 1, 1991, and June 30, 2006 (median follow-up duration, 3.2 years). Cognitive function was measured using the information-memory-concentration (IMC) section of the Blessed Dementia Rating Scale. Delirium was identified using a validated medical record review method. The rate of cognitive deterioration was contrasted using random-effects regression models. RESULTS Fifty-six percent of patients with AD developed delirium during hospitalization. The rate of cognitive deterioration before hospitalization did not differ significantly between patients who developed delirium (1.4 [95% CI, 0.7-2.1] IMC points per year) and patients who did not develop delirium (0.8 [95% CI, 0.3-1.3] IMC points per year) (P = .24). After adjusting for dementia severity, comorbidity, and demographic characteristics, patients who had developed delirium experienced greater cognitive deterioration in the year following hospitalization (3.1 [95% CI, 2.1-4.1] IMC points per year) relative to patients who had not developed delirium (1.4 [95% CI, 0.2-2.6] IMC points per year). The ratio of these changes suggests that cognitive deterioration following delirium proceeds at twice the rate in the year after hospitalization compared with patients who did not develop delirium. Patients who had developed delirium maintained a more rapid rate of cognitive deterioration throughout a 5-year period following hospitalization. Sensitivity analyses that excluded rehospitalized patients and included matching on baseline cognitive function and baseline rate of cognitive deterioration produced essentially identical results. CONCLUSIONS Delirium is highly prevalent among persons with AD who are hospitalized and is associated with an increased rate of cognitive deterioration that is maintained for up to 5 years. Strategies to prevent delirium may represent a promising avenue to explore for ameliorating cognitive deterioration in AD.
Figures
Comment in
-
Drugs may exacerbate cognitive decline after delirium in people with dementia.JAMA Intern Med. 2013 Apr 8;173(7):596-7. doi: 10.1001/jamainternmed.2013.3280. JAMA Intern Med. 2013. PMID: 23568635 No abstract available.
-
Delirium admissions in dementia.JAMA Intern Med. 2013 Apr 8;173(7):597. doi: 10.1001/jamainternmed.2013.3303. JAMA Intern Med. 2013. PMID: 23568636 No abstract available.
-
The meaning of delirium.JAMA Intern Med. 2013 Apr 8;173(7):597-9. doi: 10.1001/jamainternmed.2013.3293. JAMA Intern Med. 2013. PMID: 23568637 No abstract available.
-
The meaning of delirium-reply.JAMA Intern Med. 2013 Apr 8;173(7):597-9. doi: 10.1001/jamainternmed.2013.3788. JAMA Intern Med. 2013. PMID: 23568638 No abstract available.
References
-
- Blennow K, de Leon MJ, Zetterberg H. Alzheimer’s disease. Lancet. 2006;368:387–403. - PubMed
-
- Administration on Aging. A profile of older Americans. Washington, D.C.: Department of Health and Human Services; 2007.
-
- Cummings JL. Alzheimer’s disease. N Eng J Med. 2004;351:56–67. - PubMed
-
- Fratiglioni L. Epidemiology of Alzheimer's disease and current possibilities for prevention. Acta Neurol Scand Suppl. 1996;165:33–40. - PubMed
-
- U.S. Department of Health and Human Services. [Accessed March 1, 2012];Draft national plan to address Alzheimer’s disease. 2012 via http://aspe.hhs.gov/daltcp/napa/NatlPlan.pdf.
