

Intermittent preventive therapy for malaria during pregnancy using 2 vs 3 or more doses of sulfadoxine-pyrimethamine and risk of low birth weight in Africa: systematic review and meta-analysis
- PMID: 23403684
- PMCID: PMC4669677
- DOI: 10.1001/jama.2012.216231
Intermittent preventive therapy for malaria during pregnancy using 2 vs 3 or more doses of sulfadoxine-pyrimethamine and risk of low birth weight in Africa: systematic review and meta-analysis
Abstract
Importance: Intermittent preventive therapy with sulfadoxine-pyrimethamine to control malaria during pregnancy is used in 37 countries in sub-Saharan Africa, and 31 of those countries use the standard 2-dose regimen. However, 2 doses may not provide protection during the last 4 to 10 weeks of pregnancy, a pivotal period for fetal weight gain.
Objective: To perform a systematic review and meta-analysis of trials to determine whether regimens containing 3 or more doses of sulfadoxine-pyrimethamine for intermittent preventive therapy during pregnancy are associated with a higher birth weight or lower risk of low birth weight (LBW) (<2500 g) than standard 2-dose regimens.
Data sources and study selection: ISI Web of Knowledge, EMBASE, SCOPUS, PubMed, LILACS, the Malaria in Pregnancy Library, Cochrane CENTRAL, and trial registries from their inception to December 2012, without language restriction. Eligible studies included randomized and quasi-randomized trials of intermittent preventive therapy during pregnancy with sulfadoxine-pyrimethamine monotherapy.
Data extraction: Data were independently abstracted by 2 investigators. Relative risk (RR), mean differences, and 95% CIs were calculated with random-effects models.
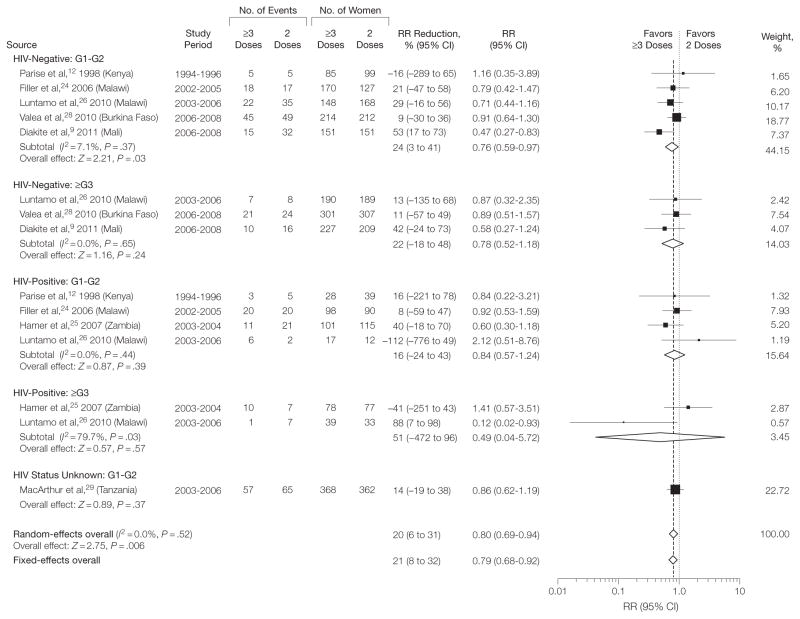
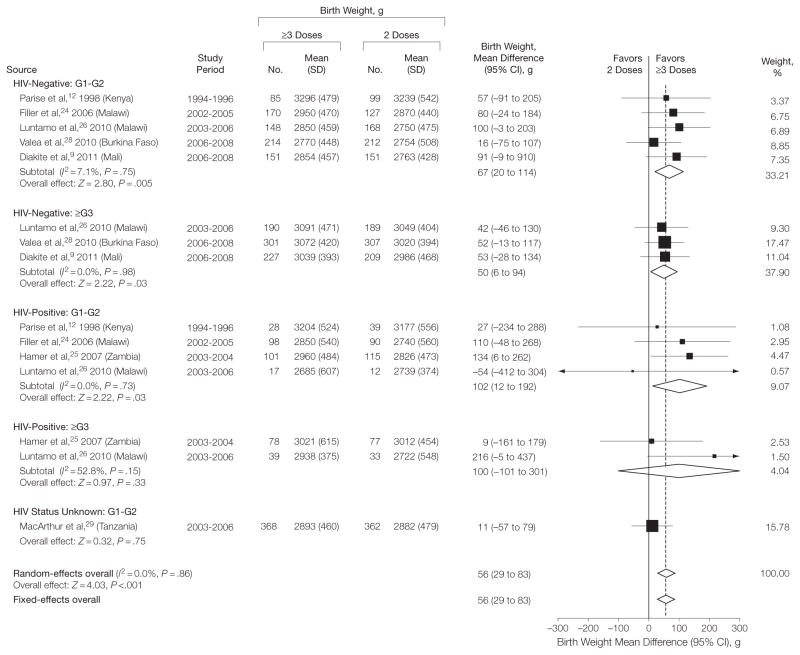
Results: Of 241 screened studies, 7 trials of 6281 pregnancies were included. The median birth weight in the 2-dose group was 2870 g (range, 2722-3239 g) and on average 56 g higher (95% CI, 29-83 g; I2 = 0%) in the ≥3-dose group. Three or more doses were associated with fewer LBW births (RR, 0.80; 95% CI, 0.69-0.94; I 2 = 0%), with a median LBW risk per 1000 women in the 2-dose group (assumed control group risk) of 167 per 1000 vs 134 per 1000 in the ≥3-dose group (absolute risk reduction, 33 per 1000 [95% CI, 10-52]; number needed to treat = 31). The association was consistent across a wide range of sulfadoxine-pyrimethamine resistance (0% to 96% dihydropteroate-synthase K540E mutations). There was no evidence of small-study bias. The ≥3-dose group had less placental malaria (RR, 0.51; 95% CI, 0.38-0.68; I 2 = 0%, in 6 trials, 63 vs 32 per 1000; absolute risk reduction, 31 per 1000 [95% CI, 20-39]). In primigravid plus secundigravid women, the risk of moderate to severe maternal anemia was lower in the ≥3-dose group (RR, 0.60; 95% CI, 0.36-0.99; I2 = 20%; in 6 trials, 36 vs 22 per 1000; absolute risk reduction, 14 per 1000 [95% CI, 0.4-23]). There were no differences in rates of serious adverse events.
Conclusions and relevance: Among pregnant women in sub-Saharan Africa, intermittent preventive therapy with 3 or more doses of sulfadoxine-pyrimethamine was associated with a higher birth weight and lower risk of LBW than the standard 2-dose regimens. These data provide support for the new WHO recommendations to provide at least 3 doses of intermittent preventive therapy during pregnancy at each scheduled antenatal care visit in the second and third trimester.
Conflict of interest statement
Figures
References
-
- Desai M, ter Kuile FO, Nosten F, et al. Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis. 2007;7(2):93–104. - PubMed
-
- Steketee RW, Nahlen BL, Parise ME, Menendez C. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64(1–2 Suppl):28–35. - PubMed
-
- World Health Organization. Malaria and HIV Interactions and Their Implications for Public Health Policy: Report of a Technical Consultation Geneva, Switzerland, 23–25 June 2004. Geneva, Switzerland: World Health Organization; 2004.
-
- World Health Organization. A Strategic Framework for Malaria Prevention and Control During Pregnancy in the African Region. Brazzaville, Africa: World Health Organization: Regional Office for Africa; 2004. AFR/MAL/04/01.
-
- World Health Organization. Recommendations on the Use of Sulfadoxine-Pyrimethamine (SP) for Intermittent Preventive Treatment During Pregnancy (IPT) in Areas of Moderate to High Resistance to SP in the African Region; October 2005. 2006 http://www.who.int/malaria/publications/atoz/who_sp_statement.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
