

Cost-effectiveness of screening strategies for identifying pediatric diabetes mellitus and dysglycemia
- PMID: 23403824
- PMCID: PMC3837695
- DOI: 10.1001/jamapediatrics.2013.419
Cost-effectiveness of screening strategies for identifying pediatric diabetes mellitus and dysglycemia
Abstract
Objective: To conduct a cost-effectiveness analysis of screening strategies for identifying children with type 2 diabetes mellitus and dysglycemia (prediabetes/diabetes).
Design: Cost simulation study.
Setting: A one-time US screening program.
Study participants: A total of 2.5 million children aged 10 to 17 years.
Intervention: Screening strategies for identifying diabetes and dysglycemia.
Main outcome measures: Effectiveness (proportion of cases identified), total costs (direct and indirect), and efficiency (cost per case identified) of each screening strategy based on test performance data from a pediatric cohort and cost data from Medicare and the US Bureau of Labor Statistics.
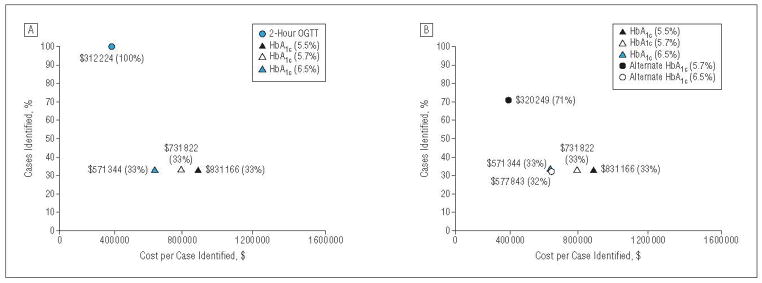
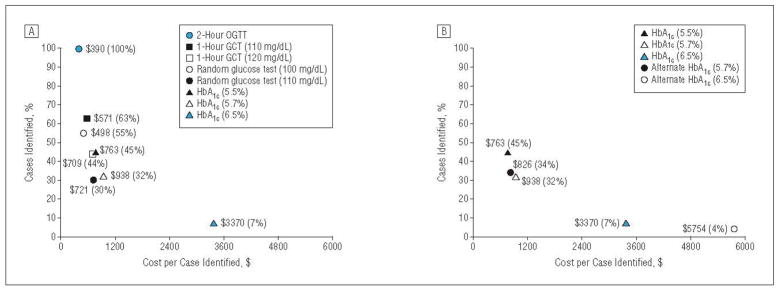
Results: In the base-case model, 500 and 400 000 US adolescents had diabetes and dysglycemia, respectively. For diabetes, the cost per case was extremely high ($312 000-$831 000 per case identified) because of the low prevalence of disease. For dysglycemia, the cost per case was in a more reasonable range. For dysglycemia, preferred strategies were the 2-hour oral glucose tolerance test (100% effectiveness; $390 per case), 1-hour glucose challenge test (63% effectiveness; $571), random glucose test (55% effectiveness; $498), or a hemoglobin A1c threshold of 5.5% (45% effectiveness; $763). Hemoglobin A1c thresholds of 5.7% and 6.5% were the least effective and least efficient (ranges, 7%-32% and $938-$3370) of all strategies evaluated. Sensitivity analyses for diabetes revealed that disease prevalence was a major driver of cost-effectiveness. Sensitivity analyses for dysglycemia did not lead to appreciable changes in overall rankings among tests.
Conclusions: For diabetes, the cost per case is extremely high because of the low prevalence of the disease in the pediatric population. Screening for diabetes could become more cost-effective if dysglycemia is explicitly considered as a screening outcome.
Conflict of interest statement
Figures
References
-
- American Diabetes Association. Type 2 diabetes in children and adolescents. Pediatrics. 2000;105(3 pt 1):671–680. - PubMed
-
- Rhodes ET, Finkelstein JA, Marshall R, Allen C, Gillman MW, Ludwig DS. Screening for type 2 diabetes mellitus in children and adolescents: attitudes, barriers, and practices among pediatric clinicians. Ambul Pediatr. 2006;6(2):110–114. - PubMed
-
- Anand SG, Mehta SD, Adams WG. Diabetes mellitus screening in pediatric primary care. Pediatrics. 2006;118(5):1888–1895. - PubMed
-
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS Data Brief. 2012;(82):1–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
