

Long term calcium intake and rates of all cause and cardiovascular mortality: community based prospective longitudinal cohort study
- PMID: 23403980
- PMCID: PMC3571949
- DOI: 10.1136/bmj.f228
Long term calcium intake and rates of all cause and cardiovascular mortality: community based prospective longitudinal cohort study
Abstract
Objective: To investigate the association between long term intake of dietary and supplemental calcium and death from all causes and cardiovascular disease.
Design: Prospective longitudinal cohort study.
Setting: Swedish mammography cohort, a population based cohort established in 1987-90.
Participants: 61 433 women (born between 1914 and 1948) followed-up for a median of 19 years.
Main outcome measures: Primary outcome measures, identified from registry data, were time to death from all causes (n=11 944) and cause specific cardiovascular disease (n=3862), ischaemic heart disease (n=1932), and stroke (n=1100). Diet was assessed by food frequency questionnaires at baseline and in 1997 for 38 984 women, and intakes of calcium were estimated. Total calcium intake was the sum of dietary and supplemental calcium.
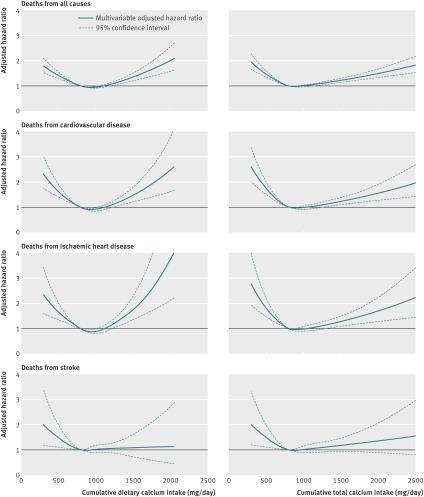
Results: The risk patterns with dietary calcium intake were non-linear, with higher rates concentrated around the highest intakes (≥1400 mg/day). Compared with intakes between 600 and 1000 mg/day, intakes above 1400 mg/day were associated with higher death rates from all causes (hazard ratio 1.40, 95% confidence interval 1.17 to 1.67), cardiovascular disease (1 49, 1.09 to 2.02), and ischaemic heart disease (2.14, 1.48 to 3.09) but not from stroke (0.73, 0.33 to 1.65). After sensitivity analysis including marginal structural models, the higher death rate with low dietary calcium intake (<600 mg/day) or with low and high total calcium intake was no longer apparent. Use of calcium tablets (6% users; 500 mg calcium per tablet) was not on average associated with all cause or cause specific mortality but among calcium tablet users with a dietary calcium intake above 1400 mg/day the hazard ratio for all cause mortality was 2.57 (95% confidence interval 1.19 to 5.55).
Conclusion: High intakes of calcium in women are associated with higher death rates from all causes and cardiovascular disease but not from stroke.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Daily calcium intake in excess of 1400 mg is associated with increased all-cause and cardiovascular disease mortality in women.Evid Based Nurs. 2014 Apr;17(2):48-9. doi: 10.1136/eb-2013-101323. Epub 2013 Jun 8. Evid Based Nurs. 2014. PMID: 23749729 No abstract available.
References
-
- Fraser WD. Hyperparathyroidism. Lancet 2009;374:145-58. - PubMed
-
- Hagstrom E, Hellman P, Larsson TE, Ingelsson E, Berglund L, Sundstrom J, et al. Plasma parathyroid hormone and the risk of cardiovascular mortality in the community. Circulation 2009;119:2765-71. - PubMed
-
- Peiris AN, Youssef D, Grant WB. Secondary hyperparathyroidism: benign bystander or culpable contributor to adverse health outcomes? South Med J 2012;105:36-42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical