

Efficacy of everolimus with exemestane versus exemestane alone in Asian patients with HER2-negative, hormone-receptor-positive breast cancer in BOLERO-2
- PMID: 23404211
- PMCID: PMC4210660
- DOI: 10.1007/s12282-013-0444-8
Efficacy of everolimus with exemestane versus exemestane alone in Asian patients with HER2-negative, hormone-receptor-positive breast cancer in BOLERO-2
Abstract
Background: The addition of mTOR inhibitor everolimus (EVE) to exemestane (EXE) was evaluated in an international, phase 3 study (BOLERO-2) in patients with hormone-receptor-positive (HR(+)) breast cancer refractory to letrozole or anastrozole. The safety and efficacy of anticancer treatments may be influenced by ethnicity (Sekine et al. in Br J Cancer 99:1757-62, 2008). Safety and efficacy results from Asian versus non-Asian patients in BOLERO-2 are reported.
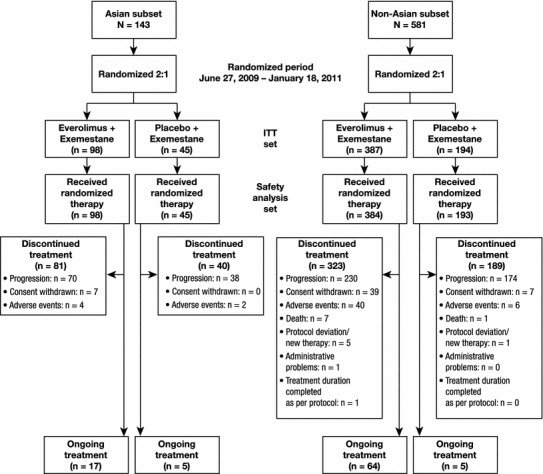
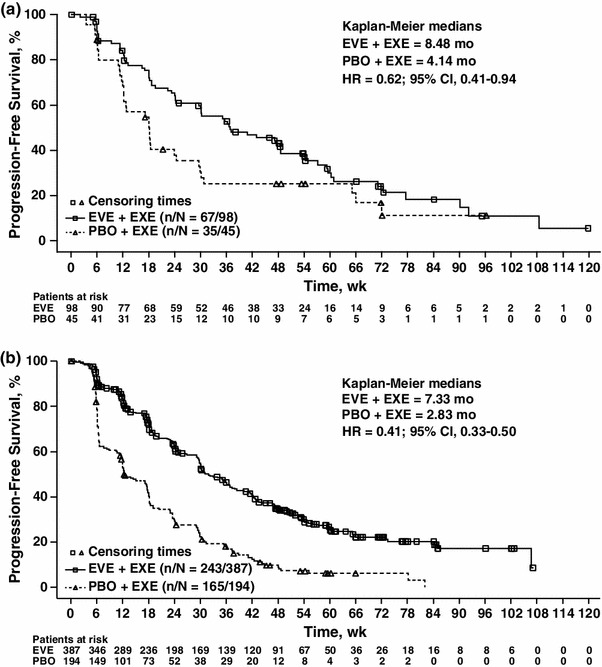
Methods: Patients were randomized (2:1) to 10 mg/day EVE + EXE or placebo (PBO) + EXE. Primary endpoint was progression-free survival (PFS). Secondary endpoints included overall survival, response rate, clinical benefit rate, and safety.
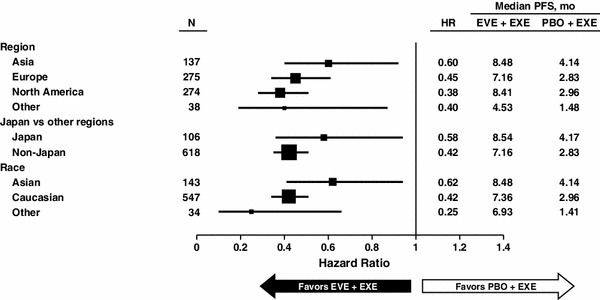
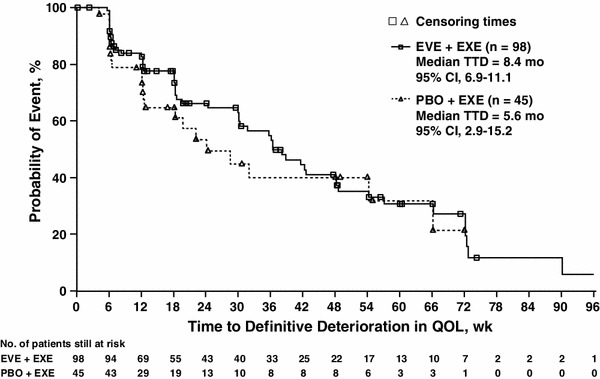
Results: Of 143 Asian patients, 98 received EVE + EXE and 45 received PBO + EXE. Treatment with EVE + EXE significantly improved median PFS versus PBO + EXE among Asian patients by 38 % (HR = 0.62; 95 % CI, 0.41-0.94). Median PFS was also improved among non-Asian patients by 59 % (HR = 0.41; 95 % CI, 0.33-0.50). Median PFS duration among EVE-treated Asian patients was 8.48 versus 4.14 months for PBO + EXE, and 7.33 versus 2.83 months, respectively, in non-Asian patients. The most common grade 3/4 adverse events (stomatitis, anemia, elevated liver enzymes, hyperglycemia, and dyspnea) occurred at similar frequencies in Asian and non-Asian patients. Grade 1/2 interstitial lung disease occurred more frequently in Asian patients. Quality of life was similar between treatment arms in Asian patients.
Conclusion: Adding EVE to EXE provided substantial clinical benefit in both Asian and non-Asian patients with similar safety profiles. This combination represents an improvement in the management of postmenopausal women with HR(+)/HER2(-) advanced breast cancer progressing on nonsteroidal aromatase inhibitors, regardless of ethnicity.
Trial registration: ClinicalTrials.gov NCT00863655.
Figures
References
-
- American Cancer Society. Global cancer facts & figures. 2nd ed. Atlanta: American Cancer Society; 2011.
-
- WHO. World Health Organization fact sheet no 297. Feb 2012. http://www.who.int/mediacentre/factsheets/fs297/en/index.html. Accessed 19 Mar 2012.
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version I.2012. Available at: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed 19 Mar 2012.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
