

The cerebellum in Parkinson's disease
- PMID: 23404337
- PMCID: PMC7273201
- DOI: 10.1093/brain/aws360
The cerebellum in Parkinson's disease
Abstract
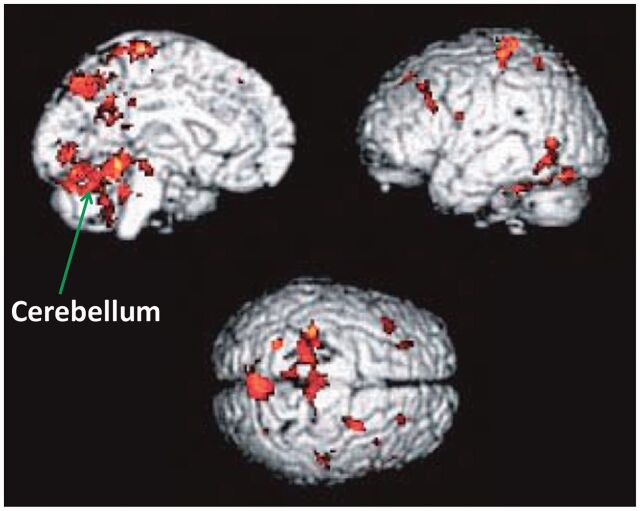
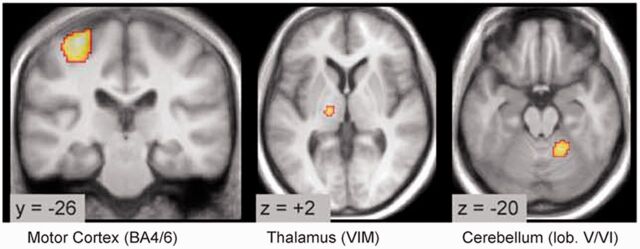
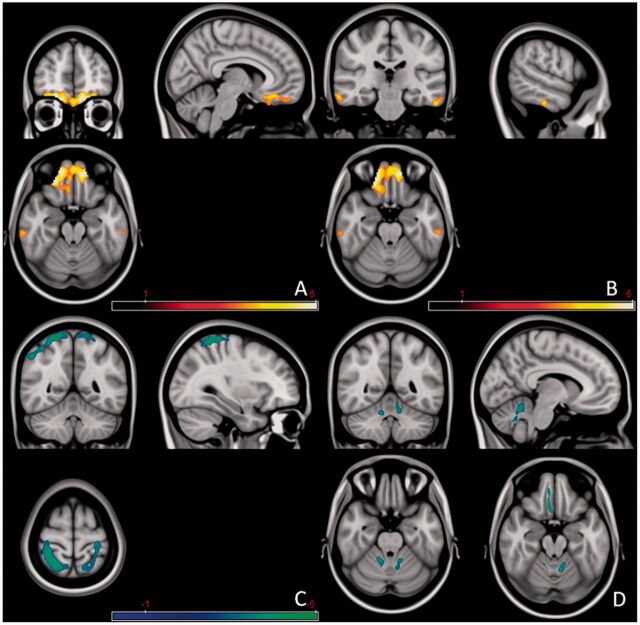
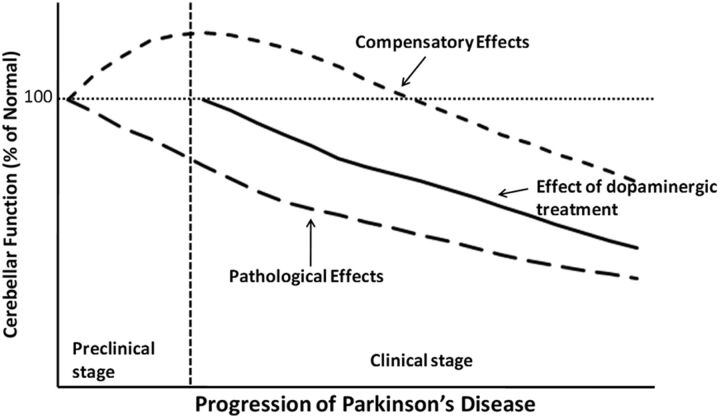
Parkinson's disease is a chronic progressive neurodegenerative disorder characterized by resting tremor, slowness of movements, rigidity, gait disturbance and postural instability. Most investigations on Parkinson's disease focused on the basal ganglia, whereas the cerebellum has often been overlooked. However, increasing evidence suggests that the cerebellum may have certain roles in the pathophysiology of Parkinson's disease. Anatomical studies identified reciprocal connections between the basal ganglia and cerebellum. There are Parkinson's disease-related pathological changes in the cerebellum. Functional or morphological modulations in the cerebellum were detected related to akinesia/rigidity, tremor, gait disturbance, dyskinesia and some non-motor symptoms. It is likely that the major roles of the cerebellum in Parkinson's disease include pathological and compensatory effects. Pathological changes in the cerebellum might be induced by dopaminergic degeneration, abnormal drives from the basal ganglia and dopaminergic treatment, and may account for some clinical symptoms in Parkinson's disease. The compensatory effect may help maintain better motor and non-motor functions. The cerebellum is also a potential target for some parkinsonian symptoms. Our knowledge about the roles of the cerebellum in Parkinson's disease remains limited, and further attention to the cerebellum is warranted.
Figures


Comment in
-
Reply: The cerebellum in Parkinson's disease and parkinsonism in cerebellar disorders.Brain. 2013 Sep;136(Pt 9):e249. doi: 10.1093/brain/awt100. Epub 2013 Jun 4. Brain. 2013. PMID: 23739172 No abstract available.
-
The cerebellum in Parkinson's disease and Parkinsonism in cerebellar disorders.Brain. 2013 Sep;136(Pt 9):e248. doi: 10.1093/brain/awt089. Epub 2013 Jun 4. Brain. 2013. PMID: 23739173 No abstract available.
References
-
- Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sorensen P. Risk of dementia in Parkinson’s disease. A community-based, prospective study. Neurology. 2001;56:730–6. - PubMed
-
- Adler CH. Nonmotor complications in Parkinson’s disease. Mov Disord. 2005;20(Suppl 11):S23–9. - PubMed
-
- Aita JF. Why patients with Parkinson's disease fall. JAMA. 1982;247:515–16. - PubMed
-
- Alexander GE, DeLong MR, Strick PL. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu Rev Neurosci. 1986;9:357–81. - PubMed
-
- Anderson VC, Burchiel KJ, Hogarth P, Farve J, Hammerstad JP. Pallidal vs. subthalamic nucleus deep brain stimulation in Parkinson's disease. Arch Neurol. 2005;62:554–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
