

Antithrombotic therapy in atrial fibrillation: aspirin is rarely the right choice
- PMID: 23404744
- PMCID: PMC3664370
- DOI: 10.1136/postgradmedj-2012-131386
Antithrombotic therapy in atrial fibrillation: aspirin is rarely the right choice
Abstract
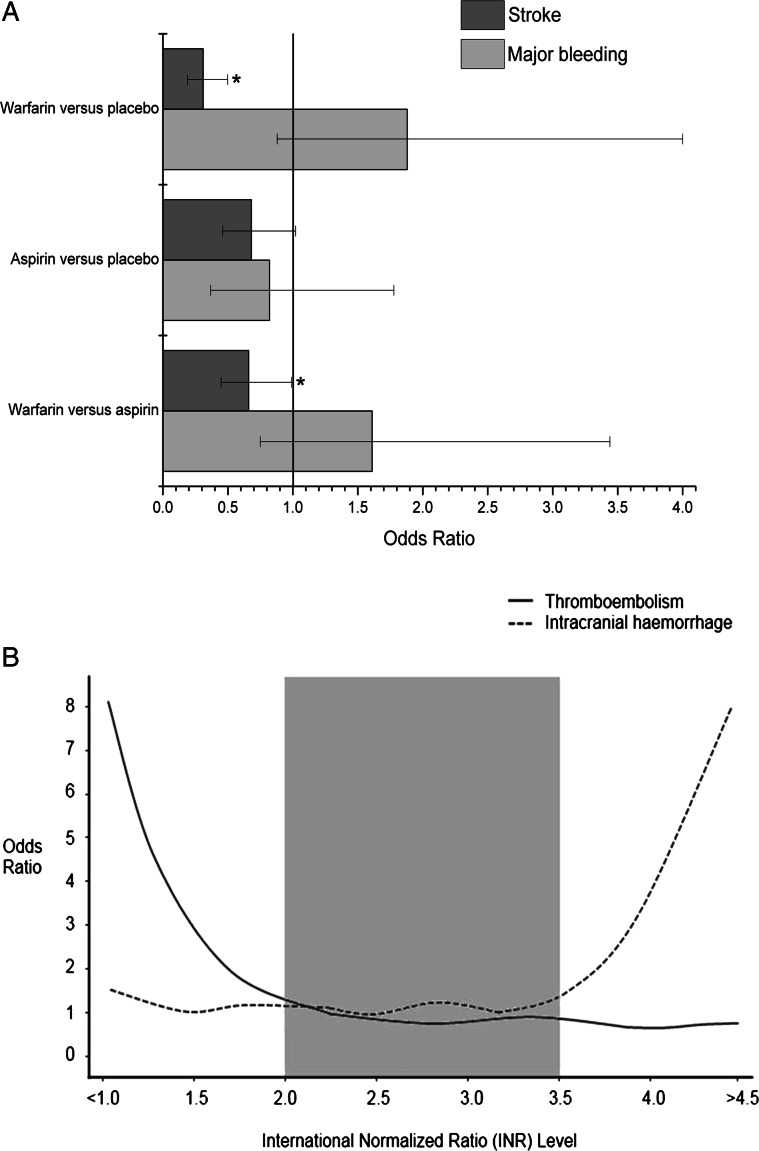
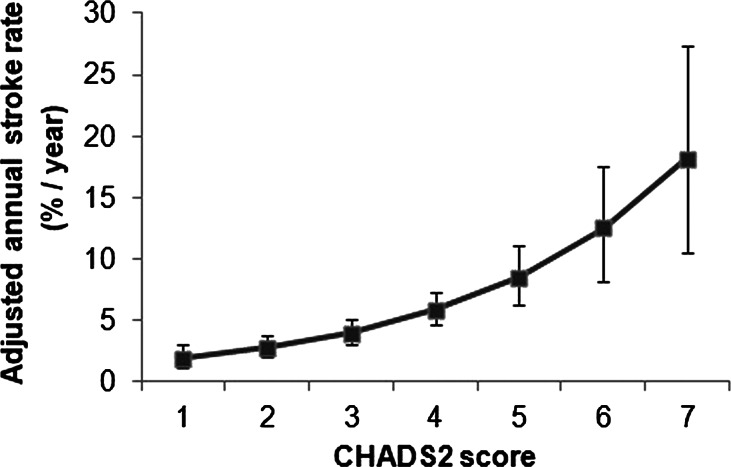
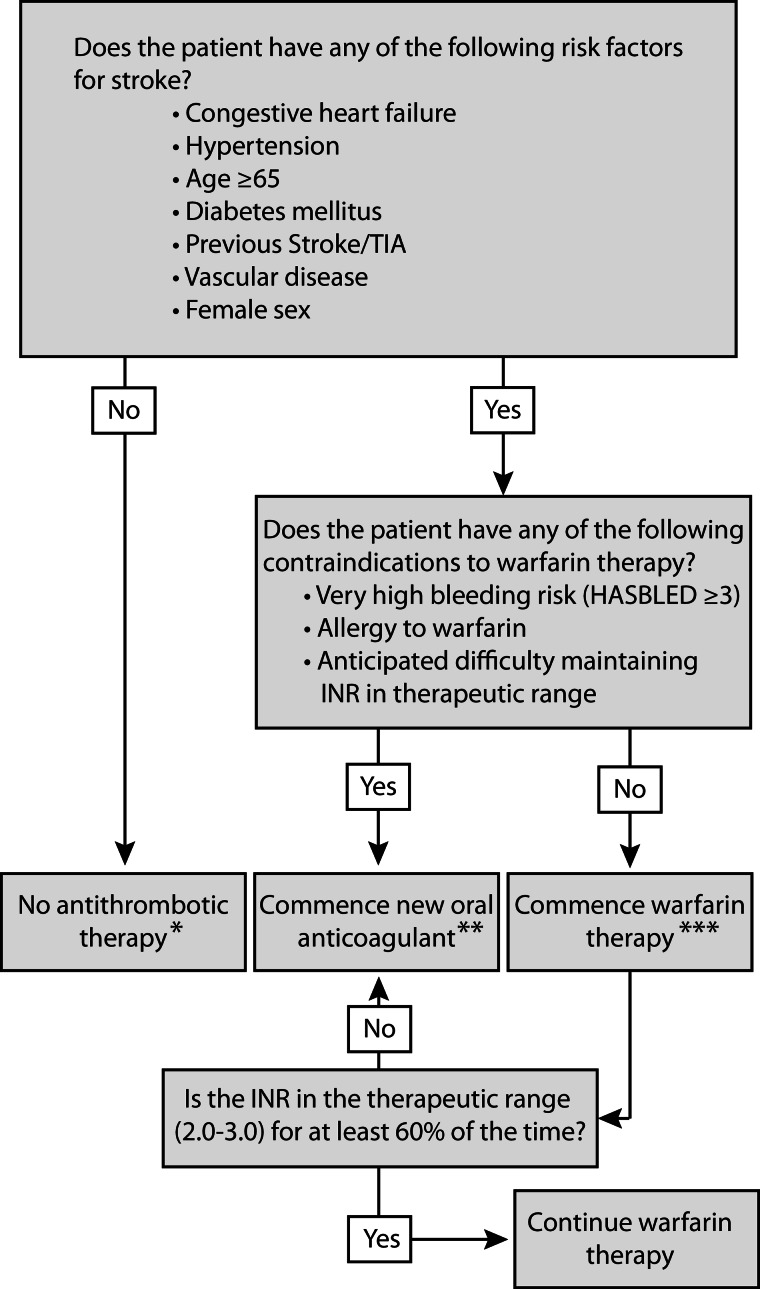
Atrial fibrillation, the commonest cardiac arrhythmia, predisposes to thrombus formation and consequently increases risk of ischaemic stroke. Recent years have seen approval of a number of novel oral anticoagulants. Nevertheless, warfarin and aspirin remain the mainstays of therapy. It is widely appreciated that both these agents increase the likelihood of bleeding: there is a popular conception that this risk is greater with warfarin. In fact, well-managed warfarin therapy (INR 2-3) has little effect on bleeding risk and is twice as effective as aspirin at preventing stroke. Patients with atrial fibrillation and a further risk factor for stroke (CHA2DS2-VASc >0) should therefore either receive warfarin or a novel oral agent. The remainder who are at the very lowest risk of stroke are better not prescribed antithrombotic therapy. For stroke prevention in atrial fibrillation; aspirin is rarely the right choice.
Keywords: Anticoagulant; Antithrombotic; Aspirin; Atrial Fibrillation; Warfarin.
Figures
Similar articles
-
Outcomes in a Warfarin-Treated Population With Atrial Fibrillation.JAMA Cardiol. 2016 May 1;1(2):172-80. doi: 10.1001/jamacardio.2016.0199. JAMA Cardiol. 2016. PMID: 27437888
-
Atrial fibrillation and acute myocardial infarction: antithrombotic therapy and outcomes.Am J Med. 2012 Sep;125(9):897-905. doi: 10.1016/j.amjmed.2012.04.006. Epub 2012 Jul 13. Am J Med. 2012. PMID: 22795814
-
Triple vs Dual Antithrombotic Therapy in Patients with Atrial Fibrillation and Coronary Artery Disease.Am J Med. 2016 Jun;129(6):592-599.e1. doi: 10.1016/j.amjmed.2015.12.026. Epub 2016 Jan 18. Am J Med. 2016. PMID: 26797080
-
Efficacy and Safety of the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients With Nonvalvular Atrial Fibrillation and Concomitant Aspirin Therapy: A Meta-Analysis of Randomized Trials.Circulation. 2018 Mar 13;137(11):1117-1129. doi: 10.1161/CIRCULATIONAHA.117.028513. Epub 2017 Nov 3. Circulation. 2018. PMID: 29101289
-
Prevention of vascular events in patients with atrial fibrillation: evidence, guidelines, and practice.J Cardiovasc Electrophysiol. 2003 Sep;14(9 Suppl):S52-5. doi: 10.1046/j.1540-8167.14.s9.2.x. J Cardiovasc Electrophysiol. 2003. PMID: 12950519 Review.
Cited by
-
The Rate of Clinical Outcomes in Atrial Fibrillation according to Antithrombotic Strategy: The COOL-AF Registry.Cardiovasc Ther. 2022 Feb 21;2022:5797257. doi: 10.1155/2022/5797257. eCollection 2022. Cardiovasc Ther. 2022. PMID: 35284003 Free PMC article.
-
Atrial fibrillation in low- and middle-income countries: a narrative review.Eur Heart J Suppl. 2020 Dec 22;22(Suppl O):O61-O77. doi: 10.1093/eurheartj/suaa181. eCollection 2020 Dec. Eur Heart J Suppl. 2020. PMID: 33380945 Free PMC article.
-
Hematoma Expansion Following Intracerebral Hemorrhage: Mechanisms Targeting the Coagulation Cascade and Platelet Activation.Curr Drug Targets. 2017;18(12):1329-1344. doi: 10.2174/1389450118666170329152305. Curr Drug Targets. 2017. PMID: 28378693 Free PMC article. Review.
-
A Cross-Sectional Study on Chinese Geriatricians' Knowledge, Attitudes, and Practices Regarding Oral Anticoagulants for Atrial Fibrillation Patients.J Multidiscip Healthc. 2025 Aug 6;18:4739-4747. doi: 10.2147/JMDH.S533158. eCollection 2025. J Multidiscip Healthc. 2025. PMID: 40791277 Free PMC article.
References
-
- Heeringa J, Van Der Kuip DAM, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J 2006;27:949–53 - PubMed
-
- Stewart S, Hart CL, Hole DJ, et al. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2002;113:359–64 - PubMed
-
- Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002;347:1825. - PubMed
-
- Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med 2002;347:1834–40 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
