

MRI evidence for altered venous drainage and intracranial compliance in mild traumatic brain injury
- PMID: 23405151
- PMCID: PMC3566196
- DOI: 10.1371/journal.pone.0055447
MRI evidence for altered venous drainage and intracranial compliance in mild traumatic brain injury
Erratum in
- PLoS One. 2013;8(12). doi:10.1371/annotation/bb7d0e00-ae4b-4ddc-af11-020d75a45a8e
Abstract
Purpose: To compare venous drainage patterns and associated intracranial hydrodynamics between subjects who experienced mild traumatic brain injury (mTBI) and age- and gender-matched controls.
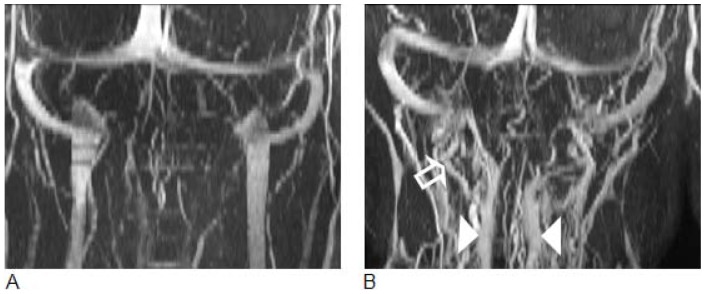
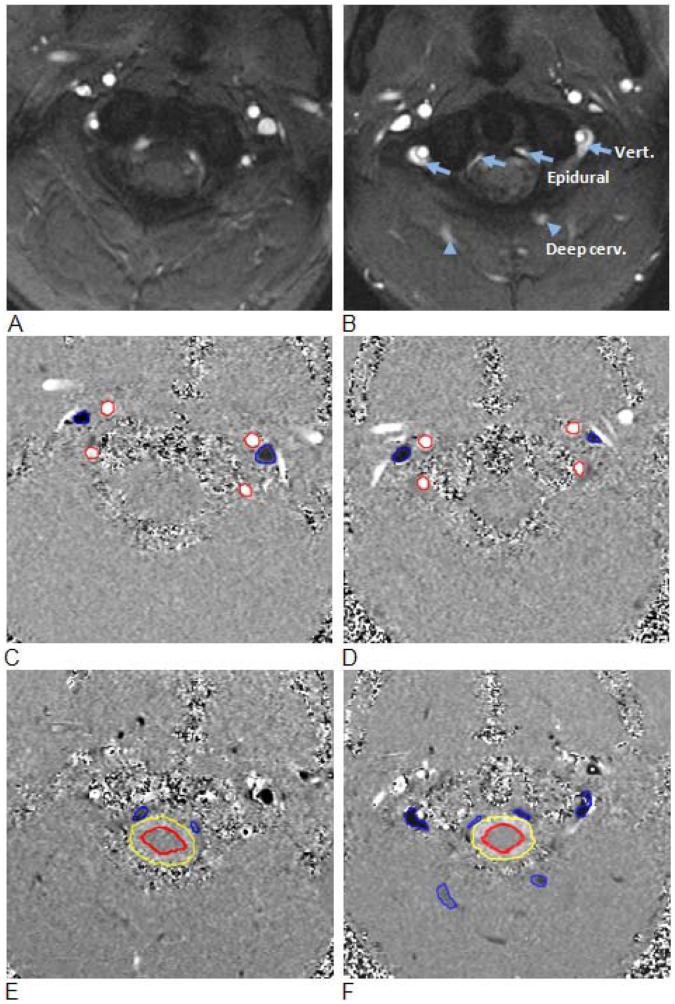
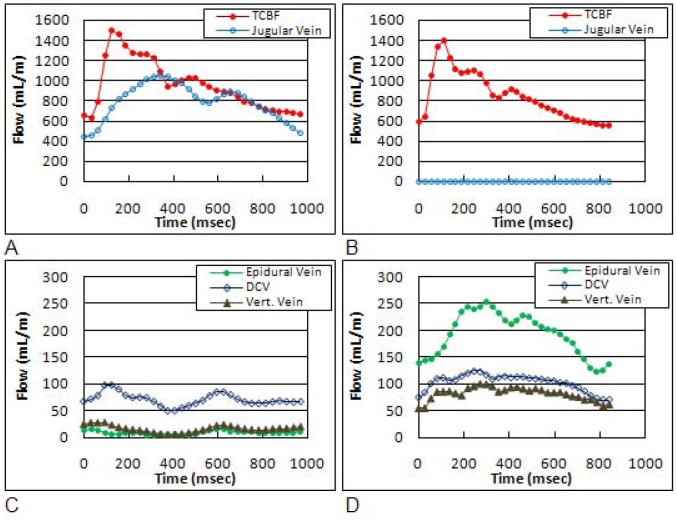
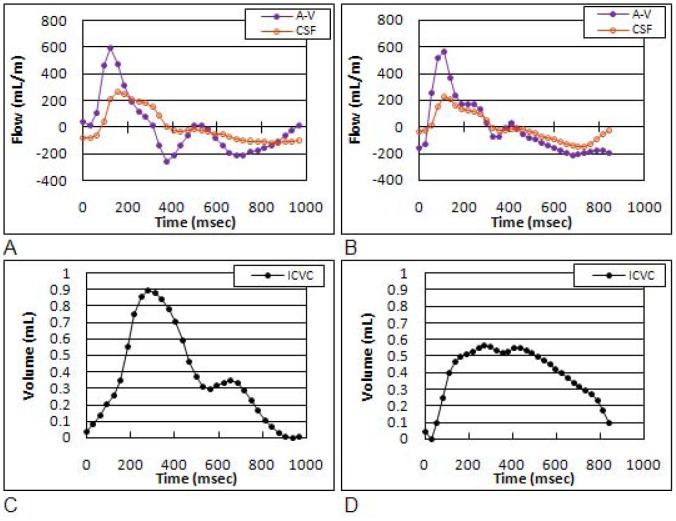
Methods: Thirty adult subjects (15 with mTBI and 15 age- and gender-matched controls) were investigated using a 3T MR scanner. Time since trauma was 0.5 to 29 years (mean 11.4 years). A 2D-time-of-flight MR-venography of the upper neck was performed to visualize the cervical venous vasculature. Cerebral venous drainage through primary and secondary channels, and intracranial compliance index and pressure were derived using cine-phase contrast imaging of the cerebral arterial inflow, venous outflow, and the craniospinal CSF flow. The intracranial compliance index is the defined as the ratio of maximal intracranial volume and pressure changes during the cardiac cycle. MR estimated ICP was then obtained through the inverse relationship between compliance and ICP.
Results: Compared to the controls, subjects with mTBI demonstrated a significantly smaller percentage of venous outflow through internal jugular veins (60.9±21% vs. controls: 76.8±10%; p = 0.01) compensated by an increased drainage through secondary veins (12.3±10.9% vs. 5.5±3.3%; p<0.03). Mean intracranial compliance index was significantly lower in the mTBI cohort (5.8±1.4 vs. controls 8.4±1.9; p<0.0007). Consequently, MR estimate of intracranial pressure was significantly higher in the mTBI cohort (12.5±2.9 mmHg vs. 8.8±2.0 mmHg; p<0.0007).
Conclusions: mTBI is associated with increased venous drainage through secondary pathways. This reflects higher outflow impedance, which may explain the finding of reduced intracranial compliance. These results suggest that hemodynamic and hydrodynamic changes following mTBI persist even in the absence of clinical symptoms and abnormal findings in conventional MR imaging.
Conflict of interest statement
Figures
References
-
- National Center for Injury Prevention and Control (2003) Report to Congress on Mild Traumatic Brain Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta, GA: Centers for Disease Control and Prevention; 2003.
-
- Kibby MY, Long CJ (1996) Minor head injury: attempts at clarifying the confusion. Brain Inj 10: 159–186. - PubMed
-
- Blumbergs PC, Scott G, Manavis J, Wainwright H, Simpson DA, et al. (1994) Staining of amyloid precursor protein to study axonal damage in mild head injury. Lancet 344: 1055–1056. - PubMed
-
- Povlishock JT, Katz DI (2005) Update of neuropathology and neurological recovery after traumatic brain injury. J Head Trauma Rehabil 20: 76–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
