

Blue light eliminates community-acquired methicillin-resistant Staphylococcus aureus in infected mouse skin abrasions
- PMID: 23406384
- PMCID: PMC3818001
- DOI: 10.1089/pho.2012.3365
Blue light eliminates community-acquired methicillin-resistant Staphylococcus aureus in infected mouse skin abrasions
Abstract
Background and objective: Bacterial skin and soft tissue infections (SSTI) affect millions of individuals annually in the United States. Treatment of SSTI has been significantly complicated by the increasing emergence of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) strains. The objective of this study was to demonstrate the efficacy of blue light (415 ± 10 nm) therapy for eliminating CA-MRSA infections in skin abrasions of mice.
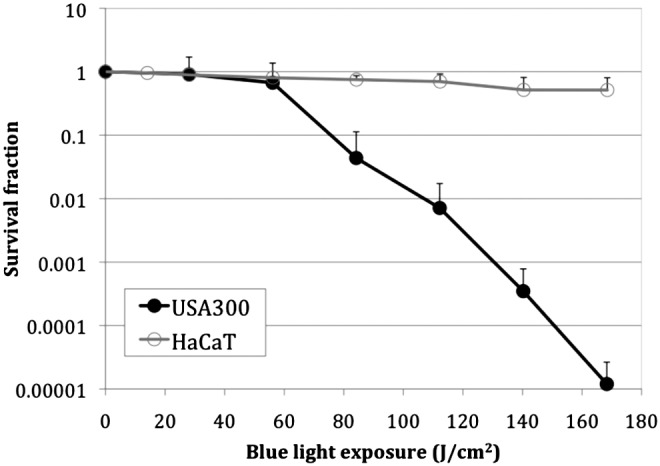
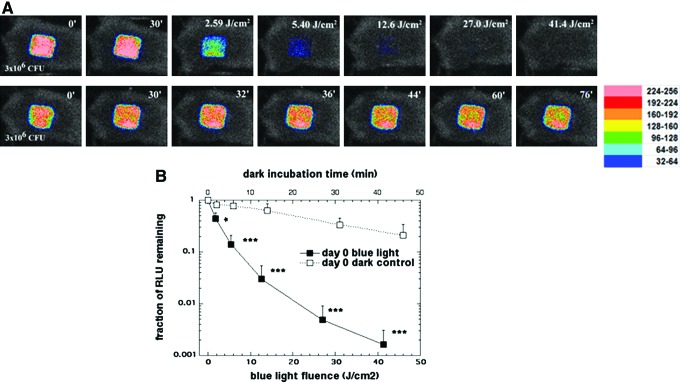
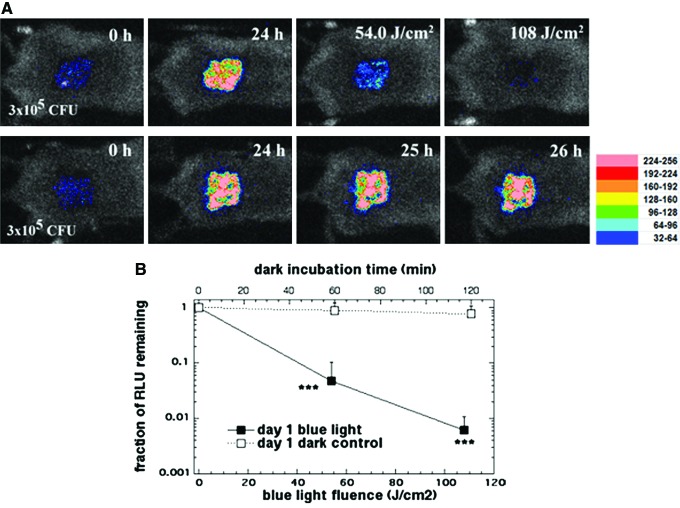
Methods: The susceptibilities of a CA-MRSA strain (USA300LAC) and human keratinocytes (HaCaT) to blue light inactivation were compared by in vitro culture studies. A mouse model of skin abrasion infection was developed using bioluminescent USA300LAC::lux. Blue light was delivered to the infected mouse skin abrasions at 30 min (acute) and 24 h (established) after the bacterial inoculation. Bioluminescence imaging was used to monitor in real time the extent of infection in mice.
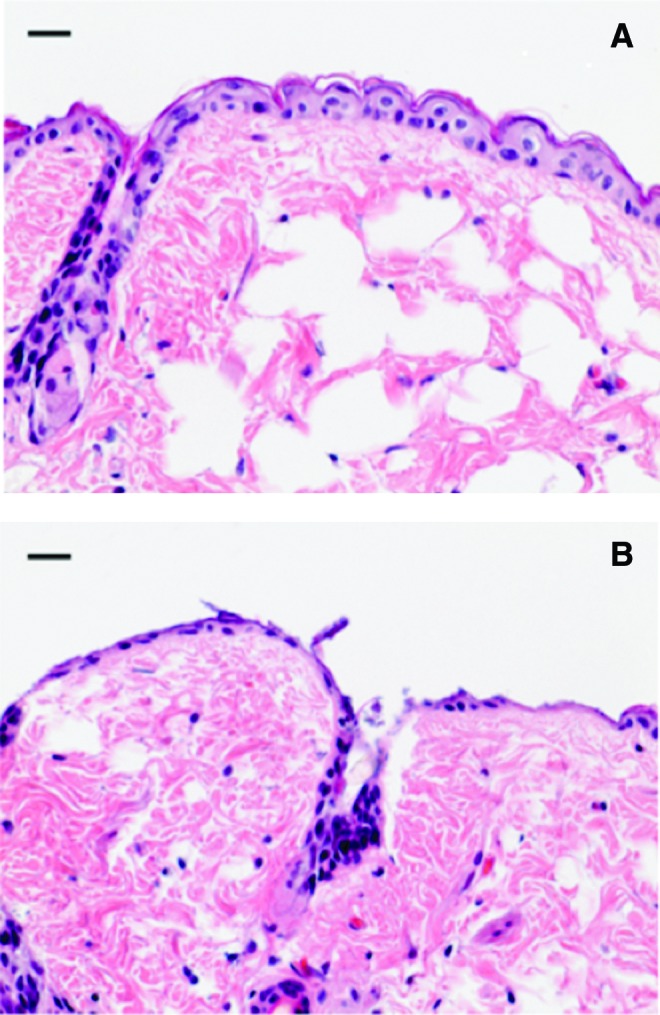
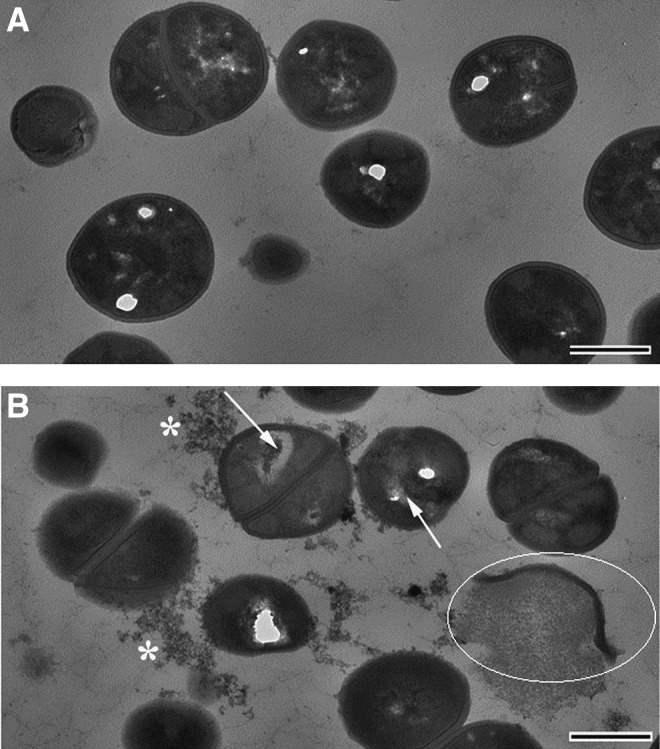
Results: USA300LAC was much more susceptible to blue light inactivation than HaCaT cells (p=0.038). Approximately 4.75-log10 bacterial inactivation was achieved after 170 J/cm(2) blue light had been delivered, but only 0.29 log10 loss of viability in HaCaT cells was observed. Transmission electron microscopy imaging of USA300LAC cells exposed to blue light exhibited disruption of the cytoplasmic content, disruption of cell walls, and cell debris. In vivo studies showed that blue light rapidly reduced the bacterial burden in both acute and established CA-MRSA infections. More than 2-log10 reduction of bacterial luminescence in the mouse skin abrasions was achieved when 41.4 (day 0) and 108 J/cm(2) (day 1) blue light had been delivered. Bacterial regrowth was observed in the mouse wounds at 24 h after the blue light therapy.
Conclusions: There exists a therapeutic window of blue light for bacterial infections where bacteria are selectively inactivated by blue light while host tissue cells are preserved. Blue light therapy has the potential to rapidly reduce the bacterial load in SSTI.
Figures
Similar articles
-
In vivo bioluminescence imaging to evaluate systemic and topical antibiotics against community-acquired methicillin-resistant Staphylococcus aureus-infected skin wounds in mice.Antimicrob Agents Chemother. 2013 Feb;57(2):855-63. doi: 10.1128/AAC.01003-12. Epub 2012 Dec 3. Antimicrob Agents Chemother. 2013. PMID: 23208713 Free PMC article.
-
Antimicrobial blue light therapy for multidrug-resistant Acinetobacter baumannii infection in a mouse burn model: implications for prophylaxis and treatment of combat-related wound infections.J Infect Dis. 2014 Jun 15;209(12):1963-71. doi: 10.1093/infdis/jit842. Epub 2013 Dec 30. J Infect Dis. 2014. PMID: 24381206 Free PMC article.
-
Photodynamic therapy for methicillin-resistant Staphylococcus aureus infection in a mouse skin abrasion model.Lasers Surg Med. 2010 Jan;42(1):38-44. doi: 10.1002/lsm.20887. Lasers Surg Med. 2010. PMID: 20077489 Free PMC article.
-
[Community-acquired methicillin-resistant Staphylococcus aureus].Enferm Infecc Microbiol Clin. 2008 Nov;26 Suppl 13:19-24. doi: 10.1157/13128776. Enferm Infecc Microbiol Clin. 2008. PMID: 19100163 Review. Spanish.
-
Current knowledge of methicillin-resistant Staphylococcus aureus and community-associated methicillin-resistant Staphylococcus aureus.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2008 Dec;152(2):191-202. doi: 10.5507/bp.2008.030. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2008. PMID: 19219207 Review.
Cited by
-
New Perspectives on Old and New Therapies of Staphylococcal Skin Infections: The Role of Biofilm Targeting in Wound Healing.Antibiotics (Basel). 2021 Nov 10;10(11):1377. doi: 10.3390/antibiotics10111377. Antibiotics (Basel). 2021. PMID: 34827315 Free PMC article. Review.
-
Blue light inactivation of the enveloped RNA virus Phi6.BMC Res Notes. 2021 May 17;14(1):187. doi: 10.1186/s13104-021-05602-y. BMC Res Notes. 2021. PMID: 34001258 Free PMC article.
-
Bioluminescent Models to Evaluate the Efficiency of Light-Based Antibacterial Approaches.Methods Mol Biol. 2022;2451:631-669. doi: 10.1007/978-1-0716-2099-1_34. Methods Mol Biol. 2022. PMID: 35505039
-
Novel approaches to the treatment of bacterial biofilm infections.Br J Pharmacol. 2017 Jul;174(14):2237-2246. doi: 10.1111/bph.13706. Epub 2017 Feb 2. Br J Pharmacol. 2017. PMID: 28063237 Free PMC article. Review.
-
Antibacterial Activity of Blue Light against Nosocomial Wound Pathogens Growing Planktonically and as Mature Biofilms.Appl Environ Microbiol. 2016 Jun 13;82(13):4006-4016. doi: 10.1128/AEM.00756-16. Print 2016 Jul 1. Appl Environ Microbiol. 2016. PMID: 27129967 Free PMC article.
References
-
- Witte W. Community-acquired methicillin-resistant Staphylococcus aureus: what do we need to know? Clin. Microbiol. Infect. 2009;15(Supp. 7):17–25. - PubMed
-
- Zervos M. Treatment options for uncomplicated community-acquired skin and soft tissue infections caused by methicillin-resistant Staphylococcus aureus: oral antimicrobial agents. Surg. Infect. (Larchmt.) 2008;9(Suppl. 1):s29–s34. - PubMed
-
- Stryjewski M.E. Chambers H.F. Skin and soft-tissue infections caused by community-acquired methicillin-resistant Staphylococcus aureus. Clin. Infect. Dis. 2008;46(Suppl. 5):S368–S377. - PubMed
-
- Graue N. Korber A. Schmid E.N. Rath P.M. Dissemond J. Therapy-resistant skin and soft tissue infections caused by community-acquired methicillin-resistant Staphylococcus aureus in a young immunocompetent adult. J. Eur. Acad. Dermatol. Venereol. 2008;22:766–767. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
