

United States multicenter study of factors predicting the persistence of GH deficiency during the transition period between childhood and adulthood
- PMID: 23406437
- PMCID: PMC3605263
- DOI: 10.1186/1687-9856-2013-6
United States multicenter study of factors predicting the persistence of GH deficiency during the transition period between childhood and adulthood
Abstract
Background: Many patients with childhood-onset growth hormone (GH) deficiency do not fulfill diagnostic criteria for GH deficiency (GHD) after attainment of adult height and may not require long-term GH treatment. Patients with history of idiopathic GHD (IGHD) pose the greatest management dilemma, as data regarding factors predictive of persistent GHD in this group are lacking.
Objectives: The objective of this study was to assess potential predictors of persistent GHD in a US patient cohort during transition from childhood to adulthood, particularly in patients with history of IGHD.
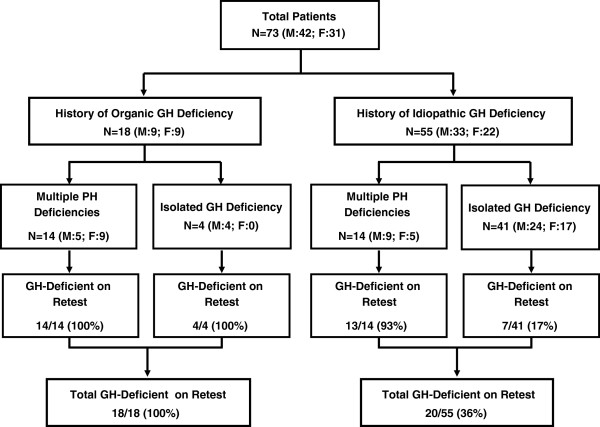
Methods: We studied 73 US patients with history of childhood-onset GHD screened at 21 US pediatric endocrine centers for a randomized clinical trial of GH replacement after attainment of adult height. The cohort comprised 42 boys/men and 31 girls/women aged14-22 years, who had received ≥1 year of GH treatment and had completed linear growth. The main outcome measures were sensitivity, specificity, positive and negative predictive values (PPV, NPV) of clinical and hormonal factors for persistent GHD (defined a priori in this study as peak GH < 5 μg/L).
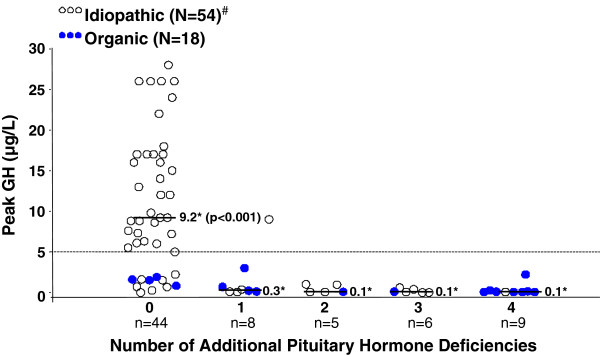
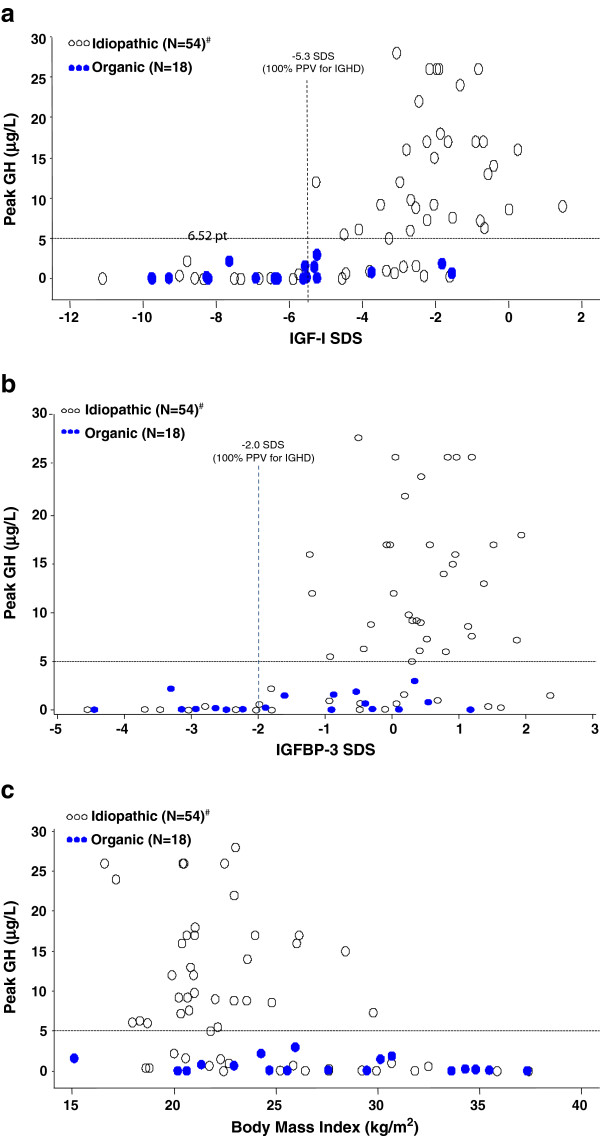
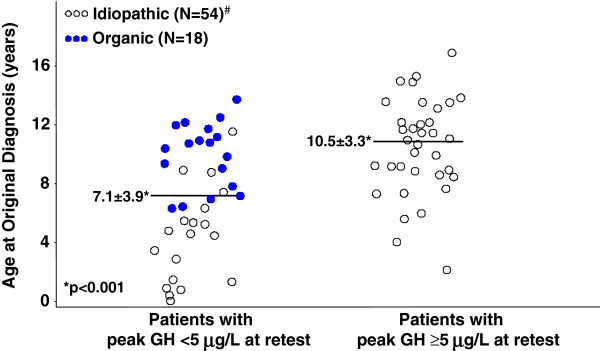
Results: For the cohort as a whole, the best predictors of persistent GHD (100% PPV) were history of organic hypothalamic-pituitary disorder or ≥2 additional pituitary hormone deficiencies (PHD). Best predictors of persistent GHD in patients with childhood history of IGHD were standard deviation scores (SDS) for serum insulin-like growth factor binding protein-3 (IGFBP-3) below -2.0, and for insulin-like growth factor-I (IGF-I) below -5.3 (measured ≥6 weeks after completion of GH treatment; PPV 100% for both), and age <4 years at original diagnosis (PPV 89%). IGF-I above -1.6 SDS had 100% NPV.
Conclusions: US patients with an organic cause of childhood-onset GHD or ≥2 additional PHDs may not require GH stimulation testing to reconfirm GHD after completion of childhood treatment. In contrast, patients with idiopathic childhood-onset GHD almost invariably require retesting, as GHD persists in only a minority (those who were very young at initial diagnosis and those who have subnormal IGFBP-3 or extremely low IGF-I after completion of childhood treatment). Subnormal posttreatment IGF-I (<-2.0 SDS) lacked predictive power for persistent GHD, whereas IGF-I > -1.6 SDS was 100% predictive of GH sufficiency.
Figures
References
-
- Colle M, Auzerie J. Discontinuation of growth hormone therapy in growth-hormone-deficient patients: assessment of body fat mass using bioelectrical impedance. Horm Res. 1993;39(5–6):192–196. - PubMed
-
- Ogle GD, Moore B, Lu PW, Craighead A, Briody JN, Cowell CT. Changes in body composition and bone density after discontinuation of growth hormone therapy in adolescence: an interim report. Acta Paediatr Suppl. 1994;399:3–7. - PubMed
-
- Attanasio AF, Lamberts SW, Matranga AM, Birkett MA, Bates PC, Valk NK, Hilsted J, Bengtsson BA, Strasburger CJ. Adult growth hormone (GH)-deficient patients demonstrate heterogeneity between childhood onset and adult onset before and during human GH treatment, Adult Growth Hormone Deficiency Study Group. J Clin Endocrinol Metab. 1997;82:82–88. doi: 10.1210/jc.82.1.82. - DOI - PubMed
-
- Gullestad L, Birkeland K, Bjonerheim R, Djoseland O, Trygstad O, Simonsen S. Exercise capacity and hormonal response in adults with childhood-onset growth hormone deficiency during long-term somatropin treatment. GH and IGF-I Res. 1998;8:377–384. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
