

Risk factors and timing of default from treatment for non-multidrug-resistant tuberculosis in Moldova
- PMID: 23407226
- PMCID: PMC3710709
- DOI: 10.5588/ijtld.12.0464
Risk factors and timing of default from treatment for non-multidrug-resistant tuberculosis in Moldova
Abstract
Setting: The Republic of Moldova, in Eastern Europe, has among the highest reported nationwide proportions of tuberculosis (TB) patients with multidrug-resistant tuberculosis (MDR-TB) worldwide. Default has been associated with increased mortality and amplification of drug resistance, and may contribute to the high MDR-TB rates in Moldova.
Objective: To assess risk factors and timing of default from treatment for non-MDR-TB from 2007 to 2010.
Design: A retrospective analysis of routine surveillance data on all non-MDR-TB patients reported.
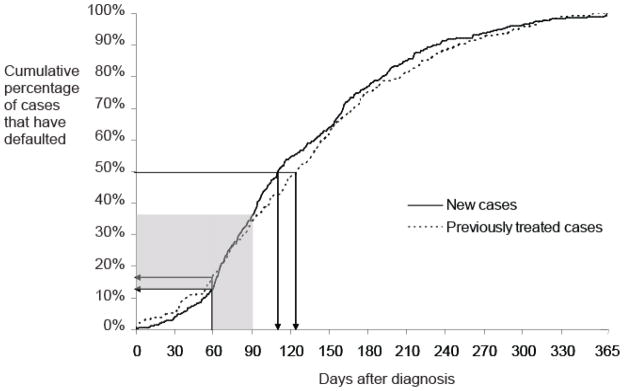
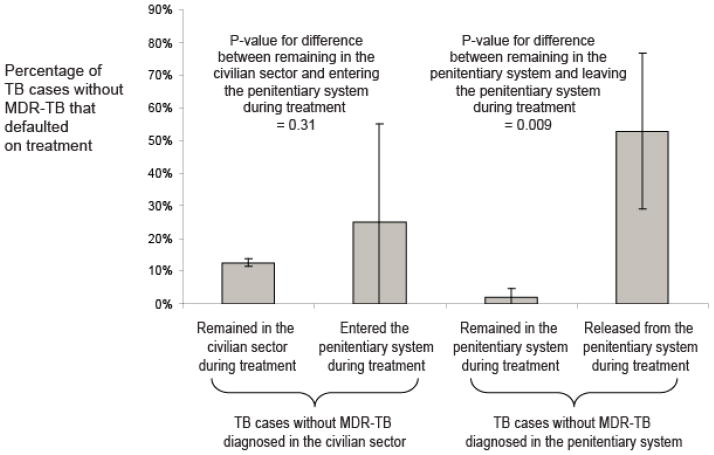
Results: A total of 14.7% of non-MDR-TB patients defaulted from treatment during the study period. Independent risk factors for default included sociodemographic factors, such as homelessness, living alone, less formal education and spending substantial time outside Moldova in the year prior to diagnosis; and health-related factors such as human immunodeficiency virus co-infection, greater lung pathology and increasing TB drug resistance. Anti-tuberculosis treatment is usually initiated within an institutional setting in Moldova, and the default risk was highest in the month following the phase of hospitalized treatment (among civilians) and after leaving prison (among those diagnosed while incarcerated).
Conclusions: Targeted interventions to increase treatment adherence for patients at highest risk of default, and improving the continuity of care for patients transitioning from institutional to community care may substantially reduce risk of default.
Conflict of interest statement
The authors have no conflicts of interest
Figures
References
-
- World Health Organization. Global Tuberculosis Control 2011. Geneva: 2011. Report No.: WHO/HTM/TB/2011.16 http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf.
-
- World Health Organization. Multidrug and extensively drug-resistant (M/XDR-TB). 2010 Global Report on Surveillance and Response. Geneva: 2010. Report No.: WHO/HTM/TB/2010.3 http://whqlibdoc.who.int/publications/2010/9789241599191_eng.pdf.
-
- Pablos-Mendez A, Knirsch CA, Barr RG, Lerner BH, Frieden TR. Nonadherence in tuberculosis treatment: predictors and consequences in New York City. Am J Med. 1997;102:164–70. - PubMed
-
- Verver S, Warren RM, Beyers N, et al. Rate of reinfection tuberculosis after successful treatment is higher than rate of new tuberculosis. Am J Respir Crit Care Med. 2005;171:1430–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
