

Accuracy of the "traffic light" clinical decision rule for serious bacterial infections in young children with fever: a retrospective cohort study
- PMID: 23407730
- PMCID: PMC3571679
- DOI: 10.1136/bmj.f866
Accuracy of the "traffic light" clinical decision rule for serious bacterial infections in young children with fever: a retrospective cohort study
Abstract
Objectives: To determine the accuracy of a clinical decision rule (the traffic light system developed by the National Institute for Health and Clinical Excellence (NICE)) for detecting three common serious bacterial infections (urinary tract infection, pneumonia, and bacteraemia) in young febrile children.
Design: Retrospective analysis of data from a two year prospective cohort study
Setting: A paediatric emergency department.
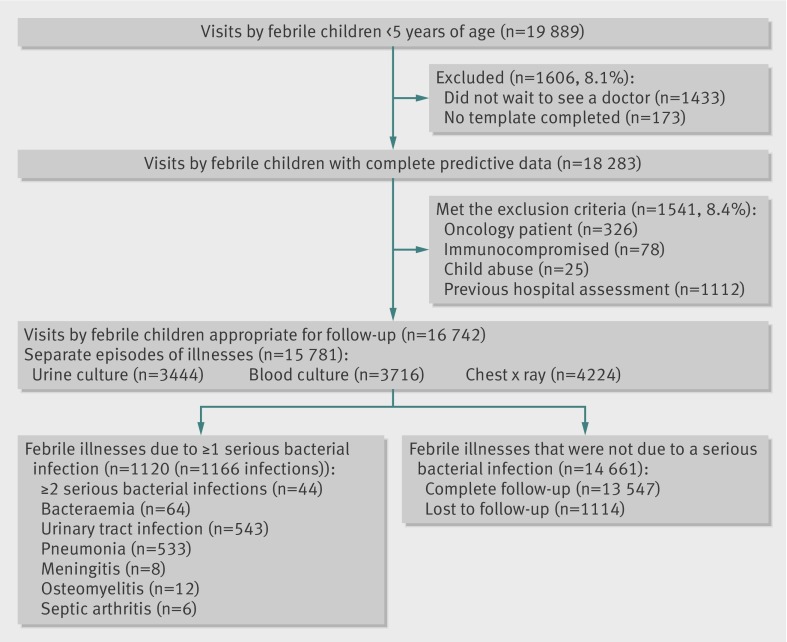
Participants: 15,781 cases of children under 5 years of age presenting with a febrile illness.
Main outcome measures: Clinical features were used to categorise each febrile episodes as low, intermediate, or high probability of serious bacterial infection (green, amber, and red zones of the traffic light system); these results were checked (using standard radiological and microbiological tests) for each of the infections of interest and for any serious bacterial infection.
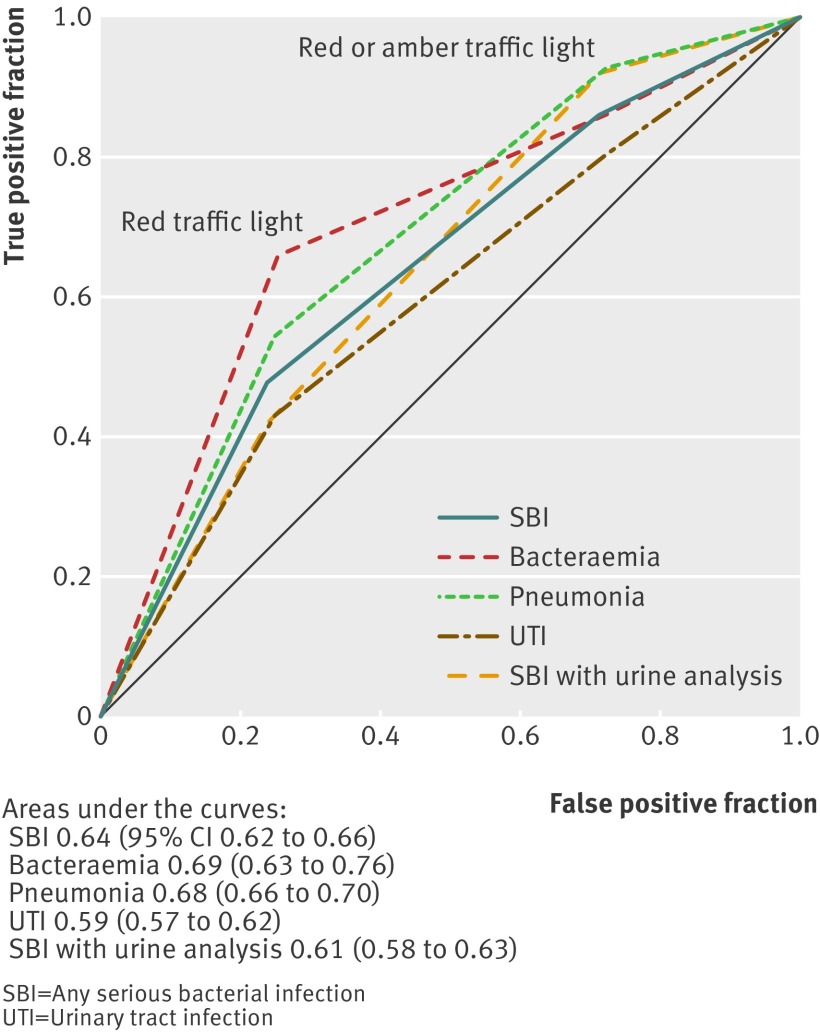
Results: After combination of the intermediate and high risk categories, the NICE traffic light system had a test sensitivity of 85.8% (95% confidence interval 83.6% to 87.7%) and specificity of 28.5% (27.8% to 29.3%) for the detection of any serious bacterial infection. Of the 1140 cases of serious bacterial infection, 157 (13.8%) were test negative (in the green zone), and, of these, 108 (68.8%) were urinary tract infections. Adding urine analysis (leucocyte esterase or nitrite positive), reported in 3653 (23.1%) episodes, to the traffic light system improved the test performance: sensitivity 92.1% (89.3% to 94.1%), specificity 22.3% (20.9% to 23.8%), and relative positive likelihood ratio 1.10 (1.06 to 1.14).
Conclusion: The NICE traffic light system failed to identify a substantial proportion of serious bacterial infections, particularly urinary tract infections. The addition of urine analysis significantly improved test sensitivity, making the traffic light system a more useful triage tool for the detection of serious bacterial infections in young febrile children.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
A frontline triage system across different health settings.BMJ. 2013 Apr 16;346:f2313. doi: 10.1136/bmj.f2313. BMJ. 2013. PMID: 23592470 No abstract available.
-
Inclusion of urine analysis not justified.BMJ. 2013 Jul 10;347:f2331. doi: 10.1136/bmj.f2331. BMJ. 2013. PMID: 23843544 No abstract available.
References
-
- Eskerud JR, Laerum E, Fagerthun H, Lunde PKM, Naess A. Fever in general practice I. Frequency and diagnoses. Fam Pract 1992;9:263-9. - PubMed
-
- Browne GJ, Currow K, Rainbow J. Practical approach to the febrile child in the emergency department. Emerg Med (Fremantle) 2001;13:426-35. - PubMed
-
- Bonadio WA, Hagen E, Rucka J, Shallow K, Stommel P, Smith D. Efficacy of a protocol to distinguish risk of serious bacterial infection in the outpatient evaluation of febrile young infants. Clin Pediatr (Phila) 1993;32:401-4. - PubMed
-
- Jaskiewicz JA, McCarthy CA, Richardson AC, White KC, Fisher DJ, Dagan R, et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics 1994;94:390-6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical