

Insights from LGI1 and CASPR2 potassium channel complex autoantibody subtyping
- PMID: 23407760
- PMCID: PMC3895328
- DOI: 10.1001/jamaneurol.2013.592
Insights from LGI1 and CASPR2 potassium channel complex autoantibody subtyping
Abstract
Objective: To determine, in patients identified as seropositive for neuronal voltage-gated potassium channel (VGKC) complex autoantibodies, the spectrum of clinical presentations and frequency of leucine-rich glioma-inactivated protein 1 (LGI1) and contactin-associated protein-like 2 (CASPR2) as defined antigenic neuronal targets in the VGKC macromolecular complex.
Design: Retrospective cohort study.
Setting: Clinical practice, Mayo Clinic Neuroimmunology Laboratory and Department of Neurology.
Patients: A total of 54 853 patients were evaluated, of whom 1992 were found to be VGKC complex IgG positive.
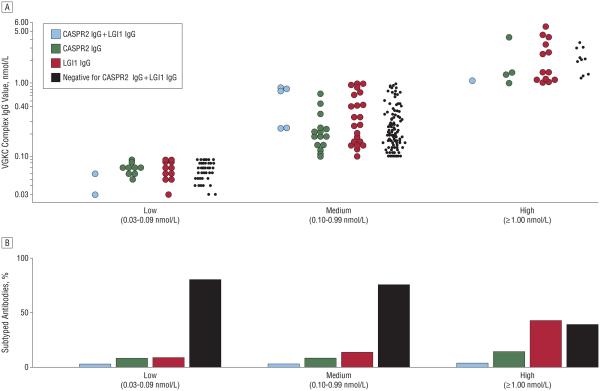
Results: From June 1, 2008, to June 30, 2010, comprehensive service serologic evaluation performed on 54853 patients with unexplained neurologic symptoms identified 1992 patients (4%) who were positive for VGKC complex IgG (values ≥ 0.03 nmol/L). Among 316 seropositive patients evaluated clinically at our institution, 82 (26%) were seropositive for LGI1 IgG and/or CASPR2 IgG. Of these 82 patients, 27% had low (0.03-0.09 nmol/L), 51% had medium (0.10-0.99 nmol/L), and 22% had high (≥ 1.00 nmol/L) VGKC complex IgG values. Leucine-rich glioma-inactivated protein 1 IgG positivity was associated with higher VGKC complex IgG values (P< .001) and cortical presentations (P< .001); CASPR2 IgG was associated with peripheral motor excitability (P= .009). However, neither autoantibody was pathognomonic for a specific neurologic presentation or correlated significantly with cancer. Neurologic phenotypes were diverse. Cerebrocortical manifestations (including cognitive impairment and seizures) were recorded in 76% of patients with LGI1 IgG alone (n=46) and 29% with CASPR2 IgG alone (n=28). Peripheral motor hyperexcitability was found in 21% of patients with CASPR2 IgG alone and 6.5% of patients with LGI1 IgG alone.
Conclusions: The study emphasizes diverse and overlapping neurologic phenotypes across a range of VGKC complex IgG values and varying LGI1 IgG and CASPR2 IgG specificities. The frequent occurrence of LGI1 IgG and CASPR2 IgG in serum samples with low and medium VGKC complex IgG values supports the clinical significance of low values in clinical evaluation. Additional antigenic components of VGKC macromolecular complexes remain to be defined.
Figures
References
-
- Shillito P, Molenaar PC, Vincent A, et al. Acquired neuromyotonia: evidence for autoantibodies directed against K+ channels of peripheral nerves. Ann Neurol. 1995;38(5):714–722. - PubMed
-
- Hart IK, Waters C, Vincent A, et al. Autoantibodies detected to expressed K+ channels are implicated in neuromyotonia. Ann Neurol. 1997;41(2):238–246. - PubMed
-
- Liguori R, Vincent A, Clover L, et al. Morvan’s syndrome: peripheral and central nervous system and cardiac involvement with antibodies to voltage-gated potassium channels. Brain. 2001;124(pt 12):2417–2426. - PubMed
-
- Josephs KA, Silber MH, Fealey RD, Nippoldt TB, Auger RG, Vernino S. Neurophysiologic studies in Morvan syndrome. J Clin Neurophysiol. 2004;21(6):440–445. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
