

Thirty-day complications after laparoscopic or open cholecystectomy: a population-based cohort study in Italy
- PMID: 23408075
- PMCID: PMC3586184
- DOI: 10.1136/bmjopen-2012-001943
Thirty-day complications after laparoscopic or open cholecystectomy: a population-based cohort study in Italy
Abstract
Objective: The objective of the study is to evaluate short-term complications after laparoscopic (LC) or open cholecystectomy (OC) in patients with gallstones by using linked hospital discharge data.
Design: Population-based cohort study.
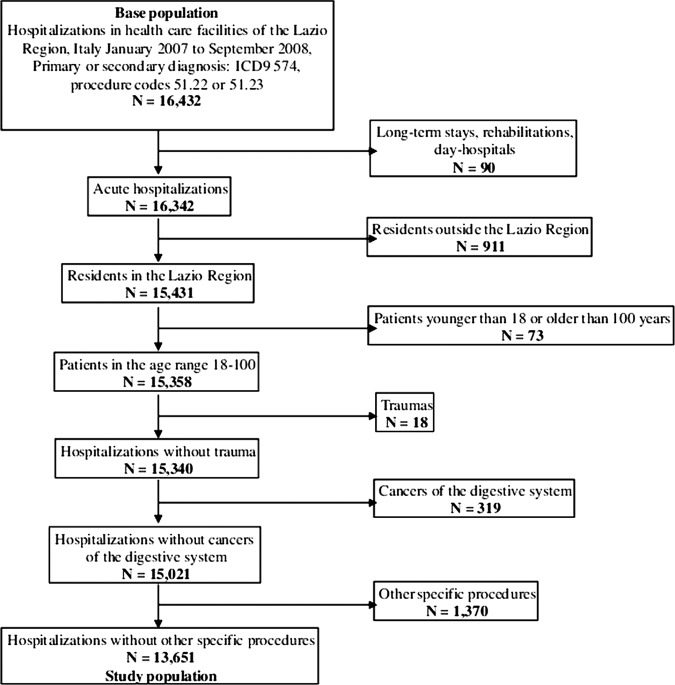
Setting: Data were obtained from the Regional Hospital Discharge Registry Lazio Region in Central Italy (around 5 million inhabitants) in 2007-2008.
Participants: All patients admitted to hospitals of Lazio with symptomatic gallstones (International Classification of disease, 9th Revision, Clinical Modification (ICD-9-CM)=574) who underwent LC (ICD-9-CM 51.23) or OC (ICD-9-CM 51.22).
Outcome measures: (1)'30-day surgical-related complications' defined as any complication of the biliary tract (including postoperative infection, haemorrhage or haematoma or seroma complicating a procedure, persistent postoperative fistula, perforation of bile duct and disruption of wound). (2) '30-day systemic complications' defined as any complications of other organs (including sepsis, infections from other organs, major cardiovascular events and selected adverse events).
Results: 13 651 patients were included; 86.1% had LC, 13.9% OC. 2.0% experienced surgical-related complications (SRC), 2.1% systemic complications (SC). The OR of complications after LC versus OC was 0.60 (p<0.001) for SRC and 0.52 (p<0.001) for SC. In relation to SRC, the advantage of LC was consistent across age categories, severity of gallstones and previous upper abdominal surgery, whereas there was no advantage among people with emergency admission (OR=0.94, p=0.764). For SC, no significant advantage of LC was seen among very old people (OR=0.99, p=0.975) and among those with previous upper abdominal surgery (OR=0.86, p=0.905).
Conclusions: This large observational study confirms that LC is more effective than OC with respect to 30-day complications. Population-based linkage of administrative datasets can enlarge evidence of treatment benefits in clinical practice.
References
-
- Madigan D, Ryan P. What can we really learn from observational studies? The need for empirical assessment of methodology for active drug safety surveillance and comparative effectiveness research. Epidemiology 2011;22:629–31 - PubMed
-
- Mullins CD, Abdulhalim AM, Lavallee DC. Continuous patient engagement in comparative effectiveness research. JAMA 2012;307:1587–8 - PubMed
-
- Agency for Health Care Research and Quality (AHRQ)—Effective Health Care Program. http://www.effectivehealthcare.ahrq.gov (accessed May 2012).
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous