

Safe, accurate, prenatal diagnosis of thanatophoric dysplasia using ultrasound and free fetal DNA
- PMID: 23408600
- PMCID: PMC4166694
- DOI: 10.1002/pd.4066
Safe, accurate, prenatal diagnosis of thanatophoric dysplasia using ultrasound and free fetal DNA
Abstract
Objective: To improve the prenatal diagnosis of thanatophoric dysplasia by defining the change in fetal size across gestation and the frequency of sonographic features, and developing non-invasive molecular genetic diagnosis based on cell-free fetal DNA (cffDNA) in maternal plasma.
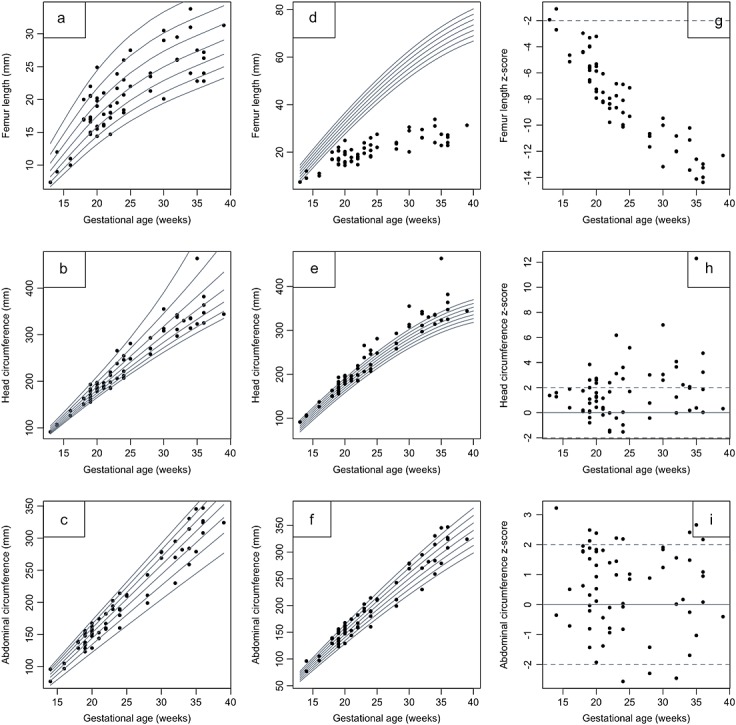
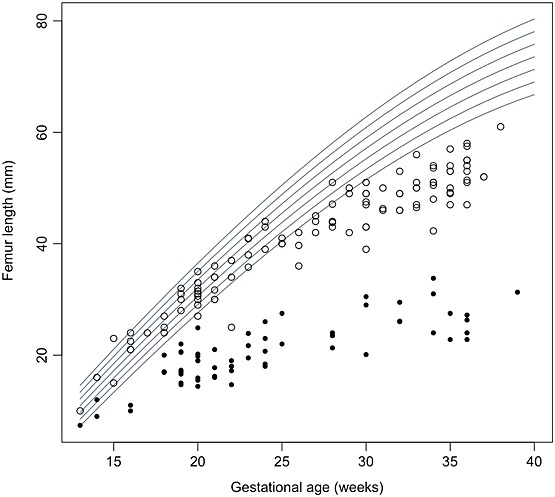
Methods: Fetuses with a confirmed diagnosis of thanatophoric dysplasia were ascertained, records reviewed, sonographic features and measurements determined. Charts of fetal size were then constructed using the LMS (lambda-mu-sigma) method and compared with charts used in normal pregnancies and those complicated by achondroplasia. Cases in this cohort referred to our Regional Genetics Laboratory for molecular diagnosis using cffDNA were identified and results reviewed.
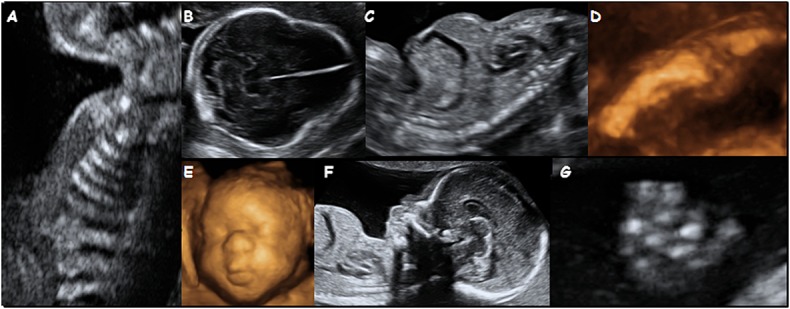
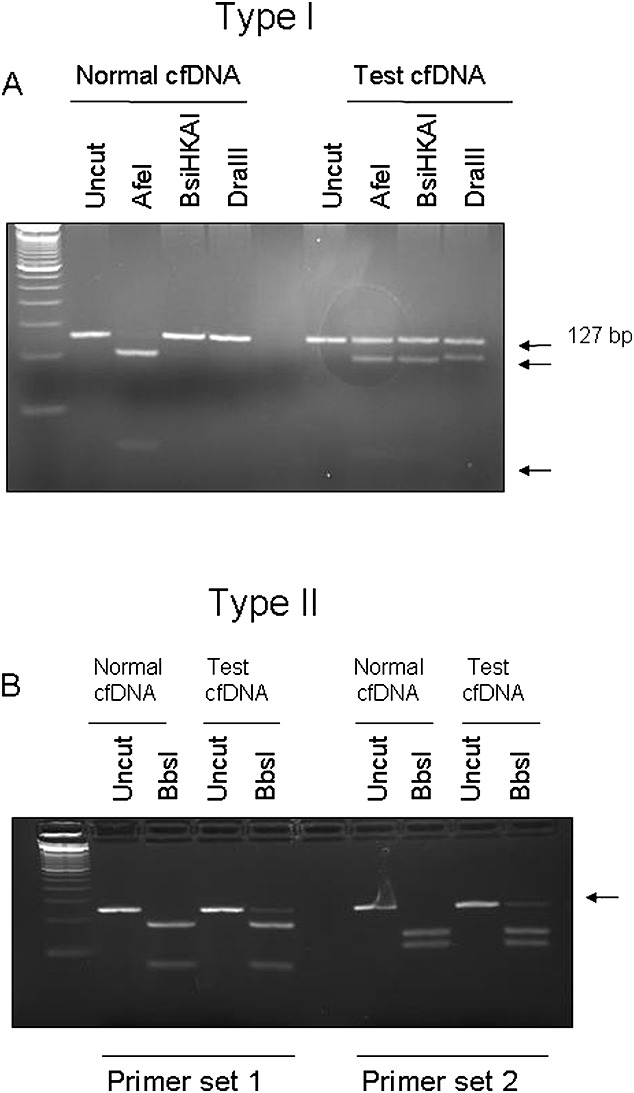
Results: Forty-two cases were scanned in our units. Commonly reported sonographic features were very short and sometimes bowed femora, frontal bossing, cloverleaf skull, short fingers, a small chest and polyhydramnios. Limb shortening was obvious from as early as 13 weeks' gestation, with minimal growth after 20 weeks. Analysis of cffDNA in three of these pregnancies confirmed the presence of the c.742C>CT (p.Arg248Cys) or the c.1948A>AG (p.Lys650Glu) mutation in the fibroblast growth factor receptor 3 gene.
Conclusion: These data should improve the accuracy of the sonographic diagnosis of thanatophoric dysplasia and have implications for reliable and safe targeted molecular confirmation using cffDNA.
© 2013 John Wiley & Sons, Ltd.
Figures
References
-
- Tavormina PL, Shiang R, Thompson LM, et al. Thanatophoric dysplasia (types I and II) caused by distinct mutations in fibroblast growth factor receptor 3. Nat Genet. 1995;9:321–8. - PubMed
-
- Wilcox WR, Tavormina PL, Krakow D, et al. Molecular, radiologic, and histopathologic correlations in thanatophoric dysplasia. Am J Med Genet. 1998;78:274–81. - PubMed
-
- Khalil A, Pajkrt E, Chitty LS. Early prenatal diagnosis of skeletal anomalies. Prenat Diagn. 2011;31:115–24. - PubMed
-
- Schramm T, Gloning KP, Minderer S, et al. Prenatal sonographic diagnosis of skeletal dysplasias. Ultrasound Obstet Gynecol. 2009;34:160–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
