

Hemostatic factors and risk of coronary heart disease in general populations: new prospective study and updated meta-analyses
- PMID: 23408959
- PMCID: PMC3567058
- DOI: 10.1371/journal.pone.0055175
Hemostatic factors and risk of coronary heart disease in general populations: new prospective study and updated meta-analyses
Abstract
Background: Activation of blood coagulation and fibrinolysis may be associated with increased risk of coronary heart disease. We aimed to assess associations of circulating tissue plasminogen activator (t-PA) antigen, D-dimer and von Willebrand factor (VWF) with coronary heart disease risk.
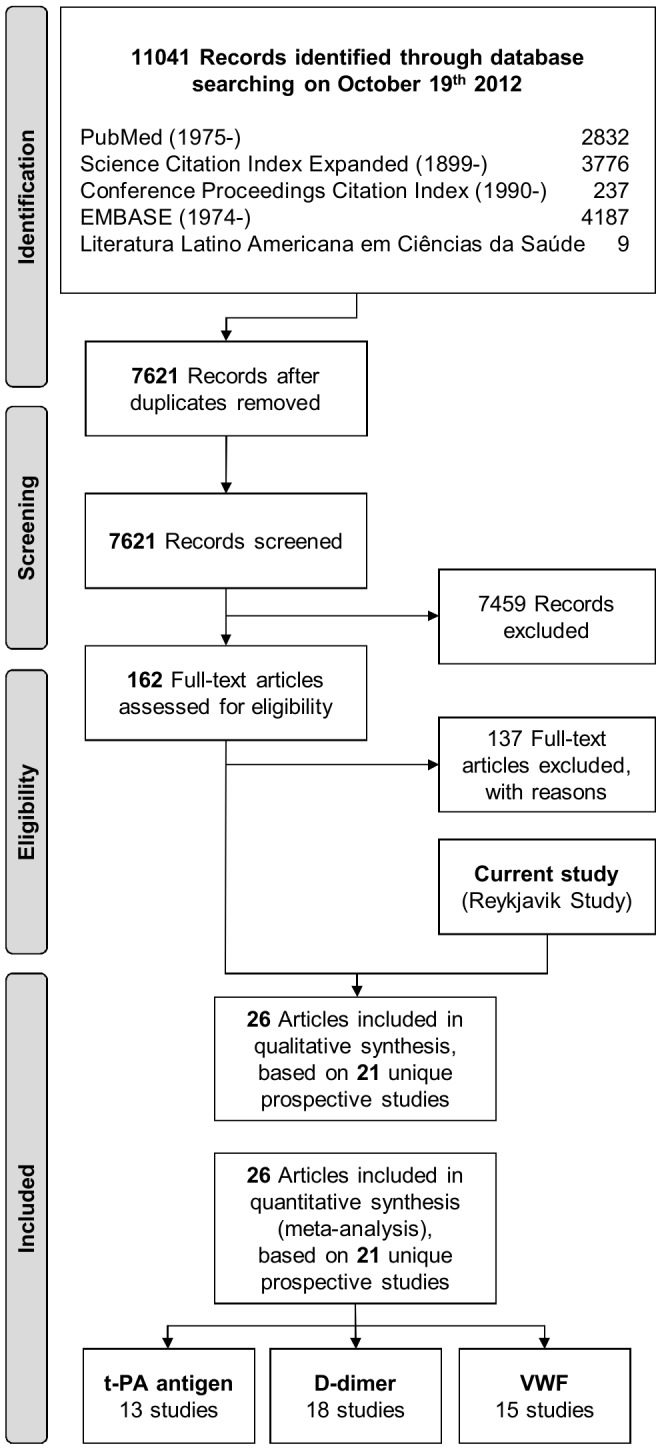
Design: Prospective case-control study, systematic review and meta-analyses.
Methods: Measurements were made in 1925 people who had a first-ever nonfatal myocardial infarction or died of coronary heart disease during follow-up (median 19.4 years) and in 3616 controls nested within the prospective population-based Reykjavik Study.
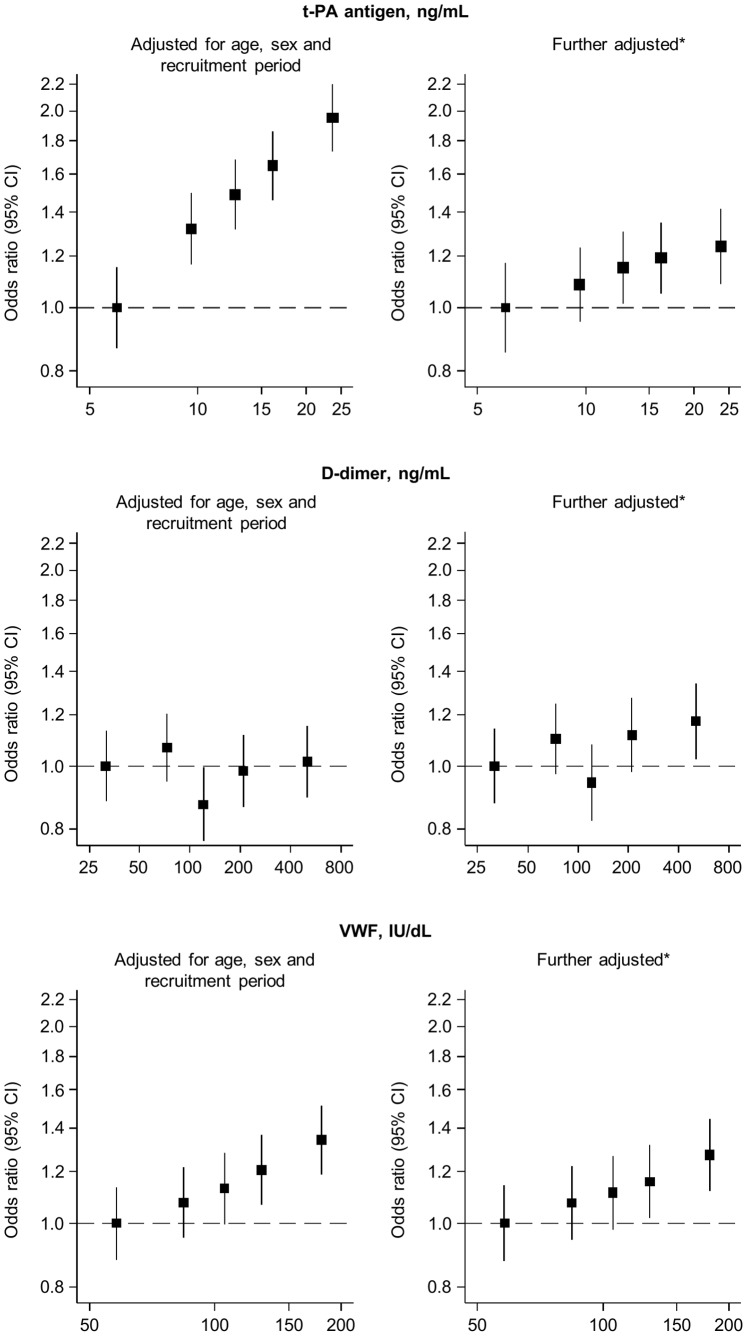
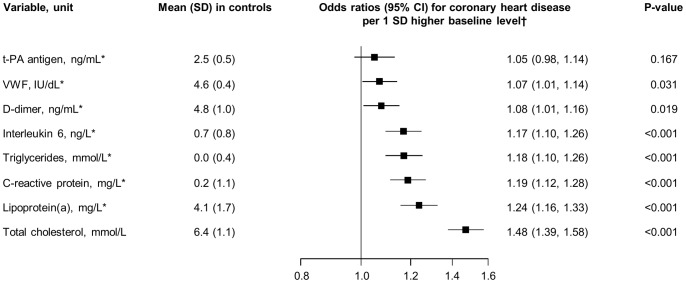
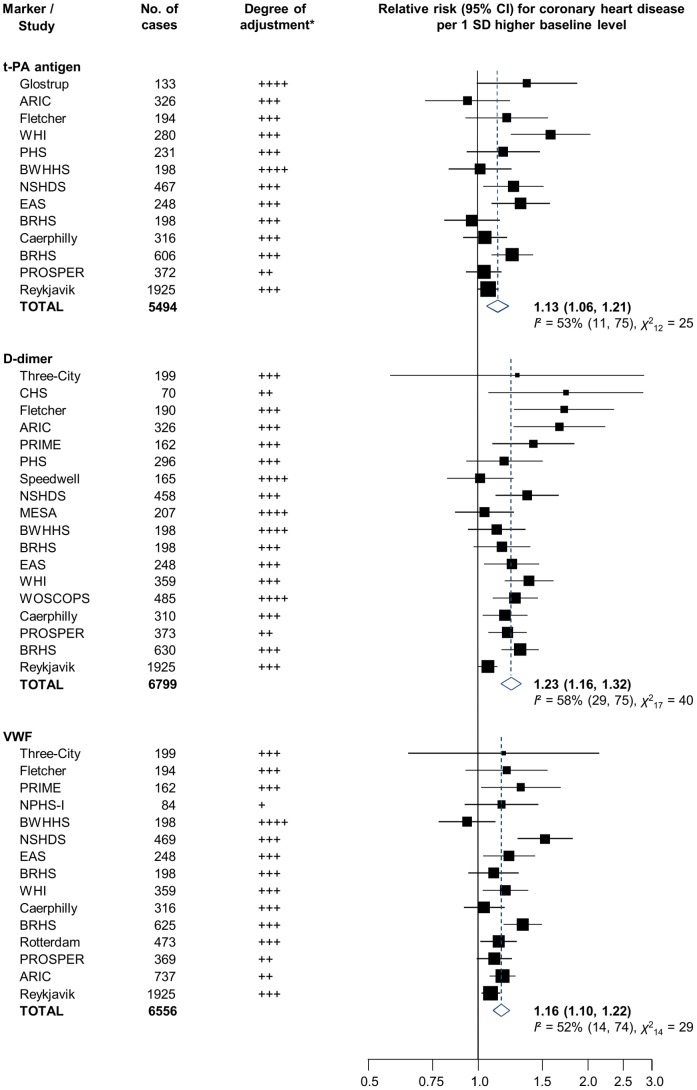
Results: Age and sex-adjusted odds ratios for coronary heart disease per 1 standard deviation higher baseline level were 1.25 (1.18, 1.33) for t-PA antigen, 1.01 (0.95, 1.07) for D-dimer and 1.11 (1.05, 1.18) for VWF. After additional adjustment for conventional cardiovascular risk factors, corresponding odds ratios were 1.07 (0.99, 1.14) for t-PA antigen, 1.06 (1.00, 1.13) for D-dimer and 1.08 (1.02, 1.15) for VWF. When combined with the results from previous prospective studies in a random-effects meta-analysis, overall adjusted odds ratios were 1.13 (1.06, 1.21) for t-PA antigen (13 studies, 5494 cases), 1.23 (1.16, 1.32) with D-dimer (18 studies, 6799 cases) and 1.16 (1.10, 1.22) with VWF (15 studies, 6556 cases).
Conclusions: Concentrations of t-PA antigen, D-dimer and VWF may be more modestly associated with first-ever CHD events than previously reported. More detailed analysis is required to clarify whether these markers are causal risk factors or simply correlates of coronary heart disease.
Conflict of interest statement
Figures
References
-
- Borissoff JI, Spronk HMH, ten Cate H (2011) The hemostatic system as a modulator of atherosclerosis. N Engl J Med 364: 1746–1760. - PubMed
-
- Lowe GDO (2006) Can haematological tests predict cardiovascular risk? The 2005 Kettle Lecture. Br J Haematol 133: 232–250. - PubMed
-
- Plow EF, Felez J, Miles LA (1991) Cellular regulation of fibrinolysis. Thromb Haemost 66: 32–36. - PubMed
-
- Nordenhem A, Wiman B (1998) Tissue plasminogen activator (tPA) antigen in plasma: correlation with different tPA/inhibitor complexes. Scand J Clin Lab Invest 58: 475–483. - PubMed
-
- Lip GY, Lowe GD (1995) Fibrin D-dimer: a useful clinical marker of thrombogenesis? Clin Sci (Lond) 89: 205–214. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
