

Microscopic-observation drug-susceptibility assay for the diagnosis of drug-resistant tuberculosis in Harare, Zimbabwe
- PMID: 23409072
- PMCID: PMC3569460
- DOI: 10.1371/journal.pone.0055872
Microscopic-observation drug-susceptibility assay for the diagnosis of drug-resistant tuberculosis in Harare, Zimbabwe
Abstract
Introduction: Limited data exist on use of the microscopic-observation drug-susceptibility (MODS) assay among persons suspected of MDR-TB living in high HIV-prevalence settings.
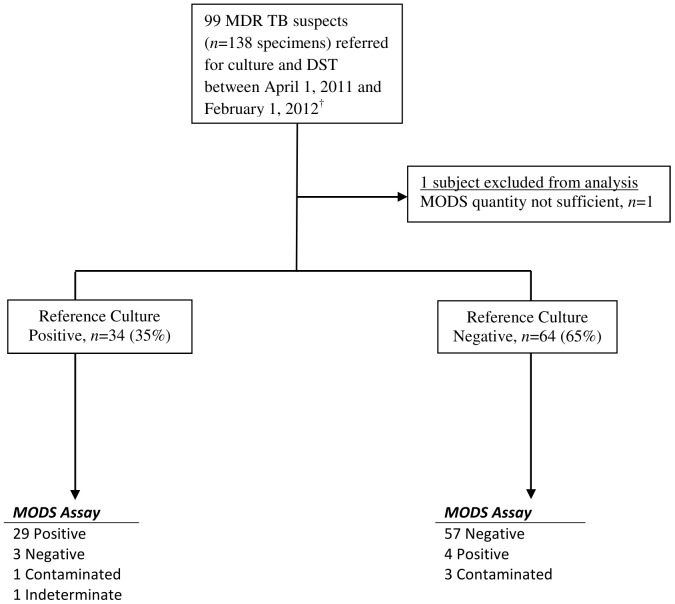
Methods: We retrospectively reviewed available clinical and drug susceptibility data for drug-resistant TB suspects referred for culture and drug-susceptibility testing between April 1, 2011 and March 1, 2012. The diagnostic accuracy of MODS was estimated against a reference standard including Löwenstein-Jensen (LJ) media and manual liquid (BACTEC MGIT) culture. The accuracy of MODS drug-susceptibility testing (DST) was assessed against a reference standard absolute concentration method.
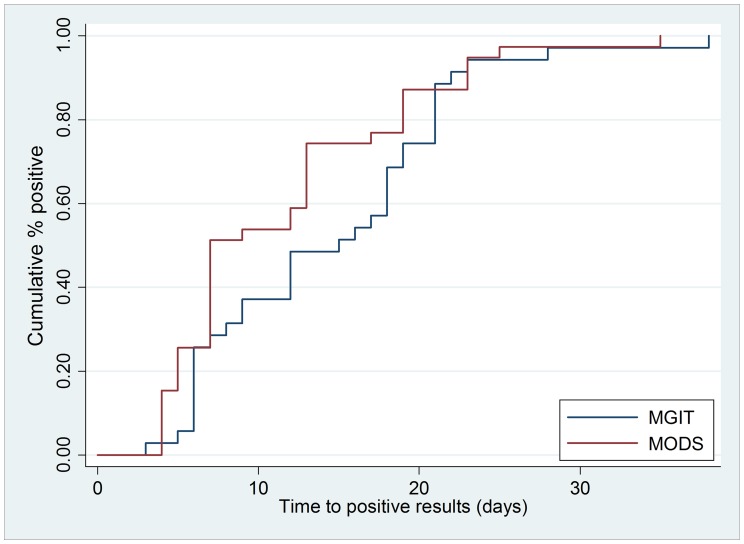
Results: One hundred thirty-eight sputum samples were collected from 99 drug-resistant TB suspects; in addition, six previously cultured MDR isolates were included for assessment of DST accuracy. Among persons with known HIV infection status, 39/59 (66%) were HIV-infected. Eighty-six percent of patients had a history of prior TB treatment, and 80% of individuals were on antituberculous treatment at the time of sample collection. M. tuberculosis was identified by reference standard culture among 34/98 (35%) MDR-TB suspects. Overall MODS sensitivity for M. tuberculosis detection was 85% (95% CI, 69-95%) and specificity was 93% (95% CI, 84-98%); diagnostic accuracy did not significantly differ by HIV infection status. Median time to positivity was significantly shorter for MODS (7 days; IQR 7-15 days) than MGIT (12 days; IQR 6-16 days) or LJ (28 days; IQR 21-35 days; p<0.001). Of 33 specimens with concurrent DST results, sensitivity of the MODS assay for detection of resistance to isoniazid, rifampin, and MDR-TB was 88% (95% CI, 68-97%), 96% (95% CI, 79-100%), and 91% (95% CI, 72-99%), respectively; specificity was 89% (95% CI, 52-100%), 89% (95% CI, 52-100%), and 90% (95% CI, 56-100%), respectively.
Conclusion: In a high HIV-prevalence setting, MODS diagnosed TB and drug-resistant TB with high sensitivity and shorter turnaround time compared with standard culture and DST methods.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of microscopic observation drug susceptibility assay for diagnosis of multidrug-resistant tuberculosis in Viet Nam.BMC Infect Dis. 2012 Mar 1;12:49. doi: 10.1186/1471-2334-12-49. BMC Infect Dis. 2012. PMID: 22375832 Free PMC article.
-
Rapid diagnosis of tuberculosis and multidrug resistance by the microscopic-observation drug-susceptibility assay.Am J Respir Crit Care Med. 2011 May 15;183(10):1427-33. doi: 10.1164/rccm.201009-1449OC. Epub 2011 Feb 4. Am J Respir Crit Care Med. 2011. PMID: 21297071
-
Evaluation of the microscopic observation drug susceptibility assay for the rapid detection of MDR-TB and XDR-TB in China: a prospective multicentre study.J Antimicrob Chemother. 2015 Feb;70(2):456-62. doi: 10.1093/jac/dku384. Epub 2014 Sep 28. J Antimicrob Chemother. 2015. PMID: 25266071
-
Non-commercial phenotypic assays for the detection of Mycobacterium tuberculosis drug resistance: a systematic review.Eur J Clin Microbiol Infect Dis. 2020 Mar;39(3):415-426. doi: 10.1007/s10096-019-03723-8. Epub 2019 Oct 30. Eur J Clin Microbiol Infect Dis. 2020. PMID: 31667670
-
Direct susceptibility testing for multi drug resistant tuberculosis: a meta-analysis.BMC Infect Dis. 2009 May 20;9:67. doi: 10.1186/1471-2334-9-67. BMC Infect Dis. 2009. PMID: 19457256 Free PMC article. Review.
Cited by
-
Performance Comparison of Three Rapid Tests for the Diagnosis of Drug-Resistant Tuberculosis.PLoS One. 2015 Aug 31;10(8):e0136861. doi: 10.1371/journal.pone.0136861. eCollection 2015. PLoS One. 2015. PMID: 26322781 Free PMC article.
-
Drug-resistant tuberculosis in high-risk groups, Zimbabwe.Emerg Infect Dis. 2014 Jan;20(1):135-7. doi: 10.3201/eid2001.130732. Emerg Infect Dis. 2014. PMID: 24377879 Free PMC article.
-
Rapid culture-based diagnosis of pulmonary tuberculosis in developed and developing countries.Front Microbiol. 2015 Nov 3;6:1184. doi: 10.3389/fmicb.2015.01184. eCollection 2015. Front Microbiol. 2015. PMID: 26579092 Free PMC article. Review.
-
Microscopic Observation Drug Susceptibility Assay for Rapid Diagnosis of Lymph Node Tuberculosis and Detection of Drug Resistance.J Clin Microbiol. 2016 Jan;54(1):185-9. doi: 10.1128/JCM.02227-15. Epub 2015 Oct 28. J Clin Microbiol. 2016. PMID: 26511739 Free PMC article.
-
Direct Determination of Pyrazinamide (PZA) Susceptibility by Sputum Microscopic Observation Drug Susceptibility (MODS) Culture at Neutral pH: the MODS-PZA Assay.J Clin Microbiol. 2020 Apr 23;58(5):e01165-19. doi: 10.1128/JCM.01165-19. Print 2020 Apr 23. J Clin Microbiol. 2020. PMID: 32132191 Free PMC article.
References
-
- World Health Organization (2012) Global Tuberculosis Report 2012. Available: http://www.who.int/tb/publications/global_report/en/. Accessed 2012 Nov 28.
-
- Gandhi NR, Moll AP, Lalloo U, Pawinski R, Zeller K, et al. (2009) Successful integration of tuberculosis and HIV treatment in rural South Africa: the Sizonq'oba study. J Acquir Immune Defic Syndr 50: 37–43. - PubMed
-
- Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, et al. (2006) Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 368: 1575–1580. - PubMed
-
- Wright A, Zignol M, Van Deun A, Falzon D, Gerdes SR, et al. (2009) Epidemiology of antituberculosis drug resistance 2002–07: an updated analysis of the Global Project on Anti-Tuberculosis Drug Resistance Surveillance. Lancet 373: 1861–1873. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
