

Social sector expenditure and child mortality in India: a state-level analysis from 1997 to 2009
- PMID: 23409166
- PMCID: PMC3567038
- DOI: 10.1371/journal.pone.0056285
Social sector expenditure and child mortality in India: a state-level analysis from 1997 to 2009
Erratum in
- PLoS One. 2013;8(4). doi: 10.1371/annotation/e917b690-4e3a-4e90-8545-d4a172617b8f doi: 10.1371/annotation/e917b690-4e3a-4e90-8545-d4a172617b8f
Abstract
Background: India is unlikely to meet the Millennium Development Goal for child mortality. As public policy impacts child mortality, we assessed the association of social sector expenditure with child mortality in India.
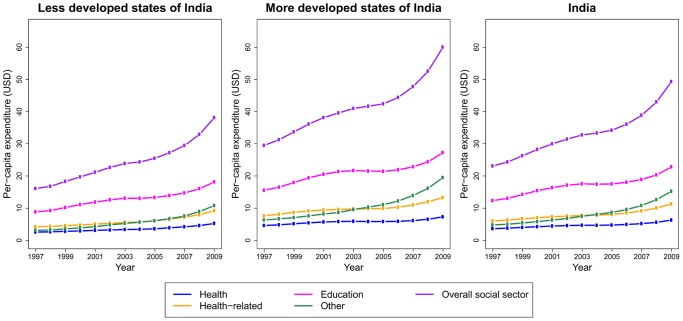
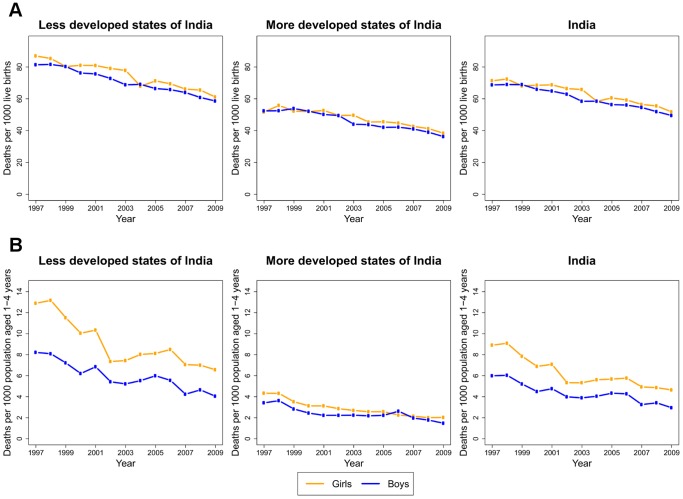
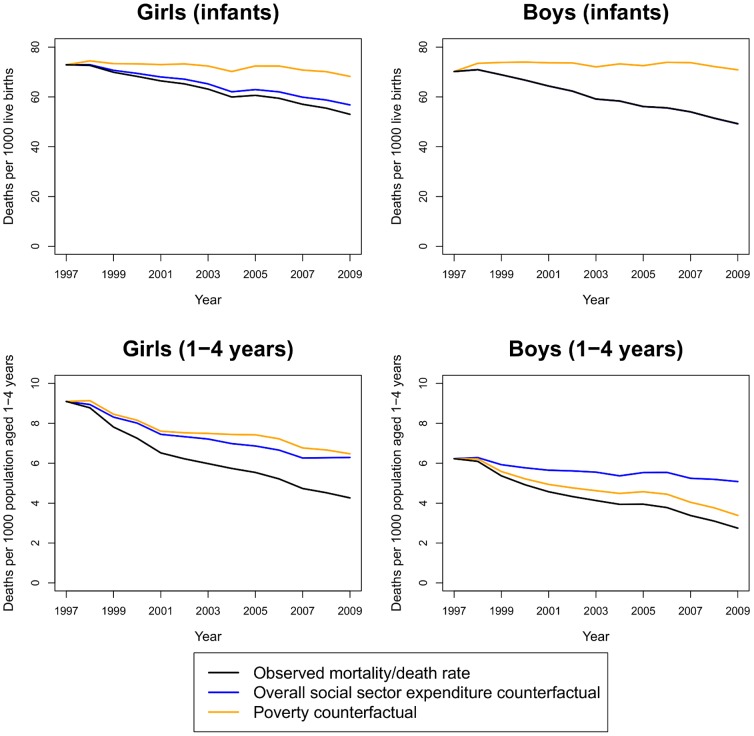
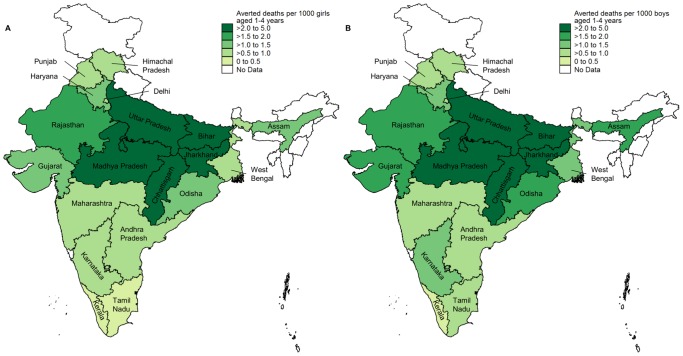
Methods and findings: Mixed-effects regression models were used to assess the relationship of state-level overall social sector expenditure and its major components (health, health-related, education, and other) with mortality by sex among infants and children aged 1-4 years from 1997 to 2009, adjusting for potential confounders. Counterfactual models were constructed to estimate deaths averted due to overall social sector increases since 1997. Increases in per capita overall social sector expenditure were slightly higher in less developed than in more developed states from 1997 to 2009 (2.4-fold versus 2-fold), but the level of expenditure remained 36% lower in the former in 2009. Increase in public expenditure on health was not significantly associated with mortality reduction in infants or at ages 1-4 years, but a 10% increase in health-related public expenditure was associated with a 3.6% mortality reduction (95% confidence interval 0.2-6.9%) in 1-4 years old boys. A 10% increase in overall social sector expenditure was associated with a mortality reduction in both boys (6.8%, 3.5-10.0%) and girls (4.1%, 0.8-7.5%) aged 1-4 years. We estimated 119,807 (95% uncertainty interval 53,409-214,662) averted deaths in boys aged 1-4 years and 94,037 (14,725-206,684) in girls in India in 2009 that could be attributed to increases in overall social sector expenditure since 1997.
Conclusions: Further reduction in child mortality in India would be facilitated if policymakers give high priority to the social sector as a whole for resource allocation in the country's 5-year plan for 2012-2017, as public expenditure on health alone has not had major impact on reducing child mortality.
Conflict of interest statement
Figures
References
-
- UNICEF (2008) State of the World's Children 2008: Child Survival. New York: UNICEF.
-
- Registrar General of India (1997–2009) Sample registration system statistical report. New Delhi: Registrar General of India.
-
- Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, et al. (2011) Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet 378: 1139–1165. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
