

Reversible tetraplegia after percutaneous nephrostolithotomy and septic shock: a case of critical illness polyneuropathy and myopathy with acute onset and complete recovery
- PMID: 23409743
- PMCID: PMC3576231
- DOI: 10.1186/1471-2369-14-36
Reversible tetraplegia after percutaneous nephrostolithotomy and septic shock: a case of critical illness polyneuropathy and myopathy with acute onset and complete recovery
Abstract
Background: Critical illness polyneuropathy (CIP) and critical illness myopathy (CIM) are complications causing weakness of respiratory and limb muscles in critically ill patients. As an important differential diagnosis of Guillain-Barré syndrome (GBS), CIP and CIM should be diagnosed with caution, after a complete clinical and laboratory examination. Although not uncommon in ICU, CIP and CIM as severe complications of percutaneous nephrostolithotomy (PNL) have not been documented in literature.
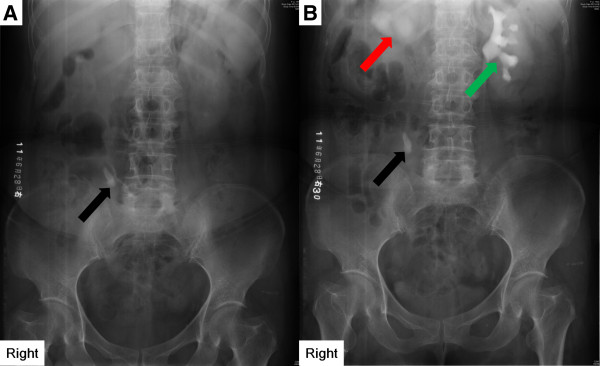
Case presentation: A 48-year-old Chinese woman was referred to our hospital, complaining of occasional pain in the right lower back for one month. Lithiasis was diagnosed by ultrasonographical and radiological examinations on the urinary system. PNL was indicated and performed. The patient developed CIP and CIM on the fourth day after PNL. Early recognition and treatment of the severe complications contributed to a satisfactory recovery of the patient.
Conclusion: This case expands our understanding of the complications of PNL and underscores the importance of differentiating CIP/CIM from GBS in case of such patients developing weakness after the treatment. Clinical characteristics and examination results should be carefully evaluated to make the diagnosis of CIP or CIM. Both anti-septic prophylaxis and control of hyperglycemia might be effective for the prevention of CIP or CIM; aggressive treatment on sepsis and multiple organ failure is considered to be the most effective measure to reduce the incidence of CIP/CIM.
Figures
Similar articles
-
Critical illness polyneuropathy and myopathy in patients with acute respiratory distress syndrome.Crit Care Med. 2005 Apr;33(4):711-5. doi: 10.1097/01.ccm.0000157969.46388.a2. Crit Care Med. 2005. PMID: 15818093
-
Long-term outcome in patients with critical illness myopathy or neuropathy: the Italian multicentre CRIMYNE study.J Neurol Neurosurg Psychiatry. 2008 Jul;79(7):838-41. doi: 10.1136/jnnp.2007.142430. Epub 2008 Mar 13. J Neurol Neurosurg Psychiatry. 2008. PMID: 18339730
-
Critical illness polyneuropathy and myopathy in a rural area in Vietnam.J Neurol Sci. 2015 Oct 15;357(1-2):276-81. doi: 10.1016/j.jns.2015.08.005. Epub 2015 Aug 5. J Neurol Sci. 2015. PMID: 26276515
-
Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis.Lancet Neurol. 2011 Oct;10(10):931-41. doi: 10.1016/S1474-4422(11)70178-8. Lancet Neurol. 2011. PMID: 21939902 Review.
-
ICU-acquired weakness: Critical illness myopathy and polyneuropathy.J Crit Care. 2025 Aug;88:155074. doi: 10.1016/j.jcrc.2025.155074. Epub 2025 Mar 29. J Crit Care. 2025. PMID: 40158422 Review.
Cited by
-
Correspondence: Guillain-Barré syndrome and hemorrhagic fever with renal syndrome.BMC Infect Dis. 2019 Aug 5;19(1):687. doi: 10.1186/s12879-019-4216-8. BMC Infect Dis. 2019. PMID: 31382899 Free PMC article.
-
Posterior Reversible Encephalopathy Syndrome and Guillain-Barré Syndrome after Head Injury: Case Report.Neurol Med Chir (Tokyo). 2018 Oct 15;58(10):453-458. doi: 10.2176/nmc.cr.2018-0049. Epub 2018 Aug 3. Neurol Med Chir (Tokyo). 2018. PMID: 30078819 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
