

Central serous chorioretinopathy: update on pathophysiology and treatment
- PMID: 23410821
- PMCID: PMC3574296
- DOI: 10.1016/j.survophthal.2012.07.004
Central serous chorioretinopathy: update on pathophysiology and treatment
Abstract
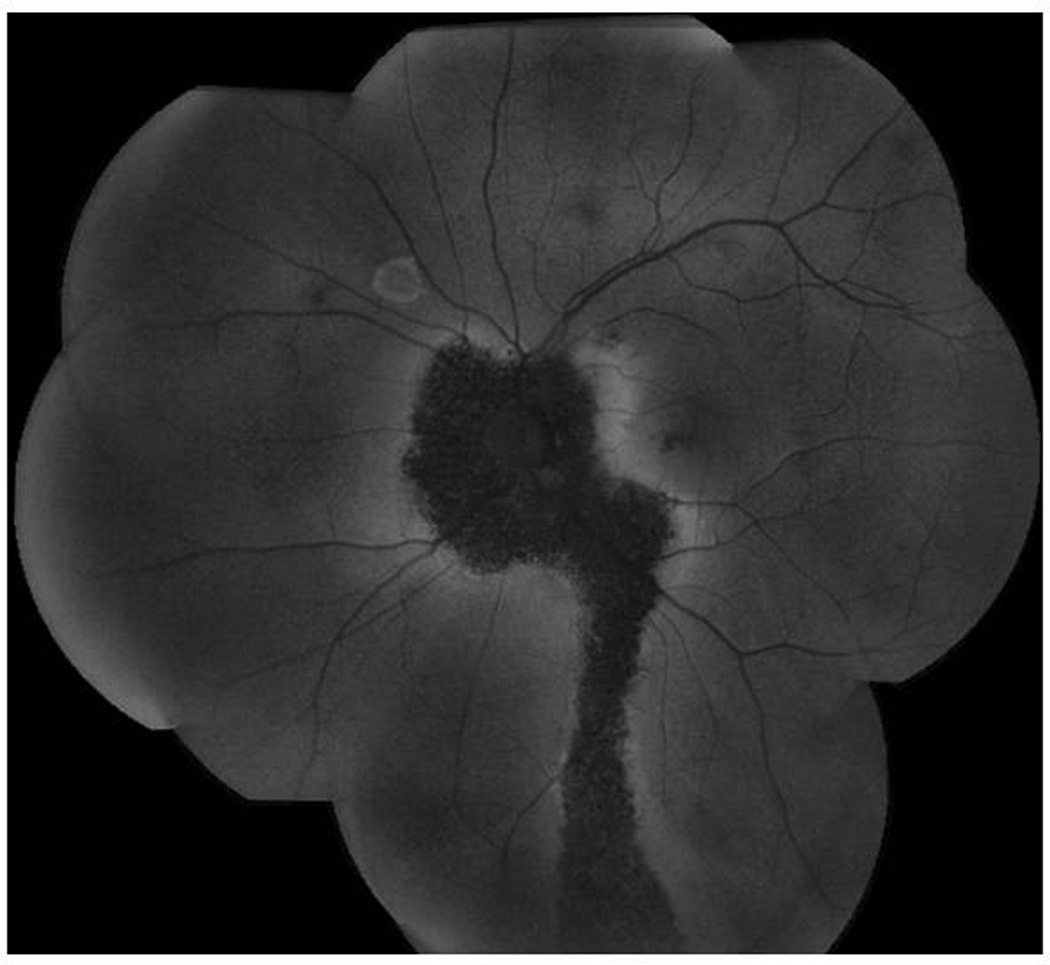
Recent technological advances--new pathophysiological insights, new imaging techniques for diagnosis and management, and new treatments--have led to an improved understanding of central serous chorioretinopathy (CSC). The primary role of the choroid has become more widely accepted with widespread use of indocyanine green angiography. Optical coherence tomography (OCT), and particularly enhanced depth imaging OCT, demonstrate a thickened and engorged choroid. Adaptive optics, fundus autofluorescence, multifocal electroretinography, microperimetry, and contrast sensitivity testing reveal that patients with even a mild course suffer previously undetected anatomic and functional loss. Although focal laser and photodynamic therapy are the current standard of care for persistent subretinal fluid in CSC, they are not appropriate in all cases, and the optimal timing of intervention remains unclear.
Published by Elsevier Inc.
Figures










References
-
- U.S. Preventive Services Task Force Ratings: Grade Definitions. Guide to Clinical Preventive Services, Third Edition: Periodic Updates. 2000–2003. [Accessed 10/10/2011]. at http://www.uspreventiveservicestaskforce.org/3rduspstf/ratings.htm.
-
- Abu el-Asrar AM. Central serous chorioretinopathy complicating systemic corticosteroid therapy. Eur J Ophthalmol. 1997;7:297–300. - PubMed
-
- Ahnoux-Zabsonre A, Quaranta M, Mauget-Faysse M. Prevalence of Helicobacter pylori in central serous chorioretinopathy and diffuse retinal epitheliopathy: a complementary study. J Fr Ophtalmol. 2004;27:1129–1133. - PubMed
-
- Aliferis K, Petropoulos IK, Farpour B, Matter MA, Safran AB. Should central serous chorioretinopathy be added to the list of ocular side effects of phosphodiesterase 5 inhibitors? Ophthalmologica. 2012;227:85–89. - PubMed
-
- Amalric P, Gourinat P, Rebiere P. Is central serous choroiditis sometimes hereditary? Bull Soc Ophtalmol Fr. 1971;71:163–168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
