

A longitudinal study of left ventricular function and structure from CKD to ESRD: the CRIC study
- PMID: 23411431
- PMCID: PMC3586970
- DOI: 10.2215/CJN.06020612
A longitudinal study of left ventricular function and structure from CKD to ESRD: the CRIC study
Abstract
Background and objectives: Abnormal left ventricular structure and function are associated with increased risk of adverse outcomes among patients with CKD and ESRD. A better understanding of changes in left ventricular mass and ejection fraction during the transition from CKD to ESRD may provide important insights to opportunities to improve cardiac outcomes.
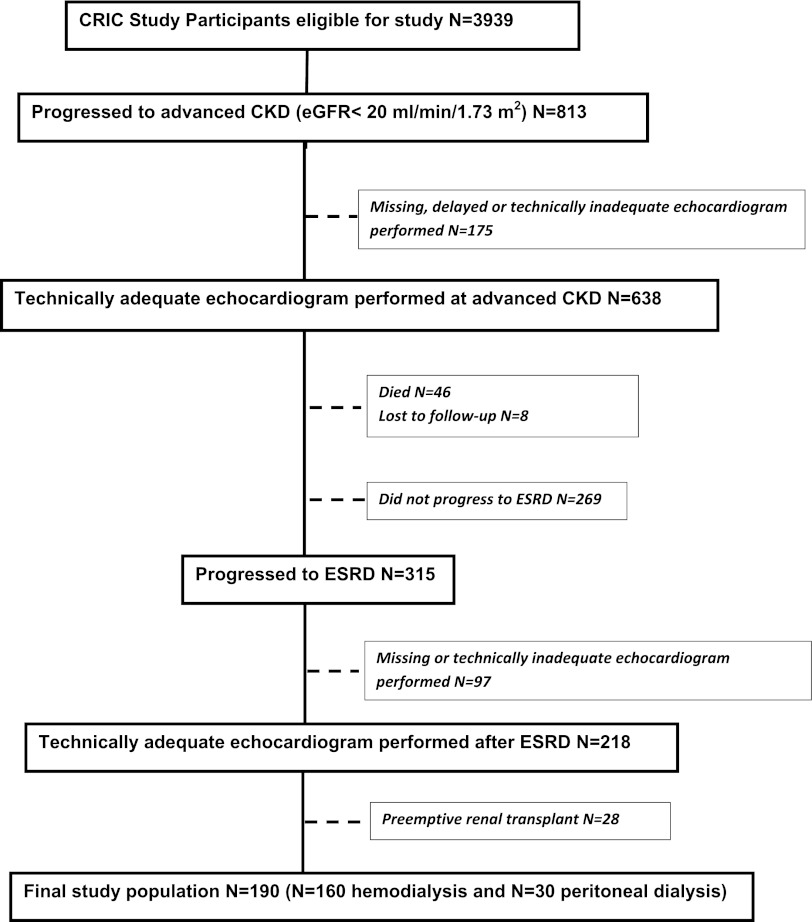
Design, setting, participants, & measurements: This was a longitudinal study of a subset of participants of the Chronic Renal Insufficiency Cohort who were enrolled from 2003 to 2007 and followed through January of 2011. Participants were included if they had serial echocardiograms performed at advanced CKD (defined as estimated GFR<20 ml/min per 1.73 m(2)) and again after ESRD (defined as need for hemodialysis or peritoneal dialysis).
Results: A total of 190 participants (44% female, 66% black) had echocardiograms during advanced CKD and after ESRD. Mean (SD) estimated GFR at advanced CKD was 16.9 (3.5) ml/min per 1.73 m(2). Mean (SD) time between the advanced CKD echocardiogram and ESRD echocardiogram was 2.0 (1.0) years. There was no significant change in left ventricular mass index (62.3-59.5 g/m(2.7), P=0.10) between advanced CKD and ESRD; however, ejection fraction significantly decreased (53%-50%, P=0.002). Interactions for age, race, dialysis modality, and diabetes status were not significant (P>0.05).
Conclusions: Mean left ventricular mass index did not change significantly from advanced CKD to ESRD; however, ejection fraction declined during this transition period. Although left ventricular mass index is fixed by advanced stages of CKD, ejection fraction decline during more advanced stages of CKD may be an important contributor to cardiovascular disease and mortality after dialysis.
Comment in
-
Echocardiography: Providing additional insights into cardiovascular structural and functional abnormalities in advanced CKD.Clin J Am Soc Nephrol. 2013 Mar;8(3):339-41. doi: 10.2215/CJN.00370113. Epub 2013 Feb 7. Clin J Am Soc Nephrol. 2013. PMID: 23393103 No abstract available.
References
-
- Herzog CA, Ma JZ, Collins AJ: Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med 339: 799–805, 1998 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, Barre PE: Impact of hypertension on cardiomyopathy, morbidity and mortality in end-stage renal disease. Kidney Int 49: 1379–1385, 1996 - PubMed
-
- Parfrey PS, Foley RN, Harnett JD, Kent GM, Murray DC, Barre PE: Outcome and risk factors for left ventricular disorders in chronic uraemia. Nephrol Dial Transplant 11: 1277–1285, 1996 - PubMed
Publication types
MeSH terms
Grants and funding
- U01DK061022/DK/NIDDK NIH HHS/United States
- K23DK088865/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01DK060980/DK/NIDDK NIH HHS/United States
- P30GM103337/GM/NIGMS NIH HHS/United States
- U01DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- K23 DK088865/DK/NIDDK NIH HHS/United States
- U01DK060902/DK/NIDDK NIH HHS/United States
- R01DK070939/DK/NIDDK NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 RR-025005/RR/NCRR NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- UL1 RR-024131/RR/NCRR NIH HHS/United States
- R01 DK070939/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- K24DK092291/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- UL1RR024986/RR/NCRR NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- U01DK061021/DK/NIDDK NIH HHS/United States
- U01DK060984/DK/NIDDK NIH HHS/United States
- UL1RR029879/RR/NCRR NIH HHS/United States
- U01DK060990/DK/NIDDK NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- M01 RR-16500/RR/NCRR NIH HHS/United States
- K24 DK092291/DK/NIDDK NIH HHS/United States
- UL1 RR-024134/RR/NCRR NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
