

Distensibility of the esophagogastric junction assessed with the functional lumen imaging probe (FLIP™) in achalasia patients
- PMID: 23413801
- PMCID: PMC3789137
- DOI: 10.1111/nmo.12097
Distensibility of the esophagogastric junction assessed with the functional lumen imaging probe (FLIP™) in achalasia patients
Abstract
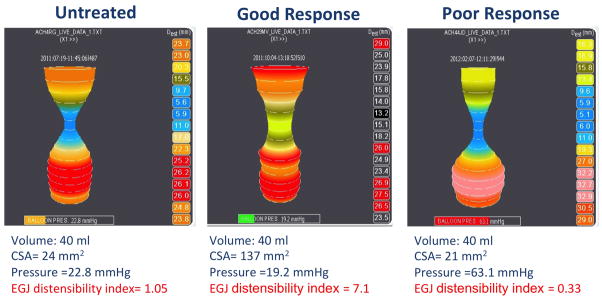
Background: The functional lumen imaging probe (FLIP), measures esophagogastric junction (EGJ) distensibility (cross-sectional area/luminal pressure) during volume-controlled distension. The aim of this study is to apply this tool to the assessment of the EGJ in untreated and treated achalasia patients and to compare EGJ distensibility with other diagnostic tools utilized in managing achalasia.
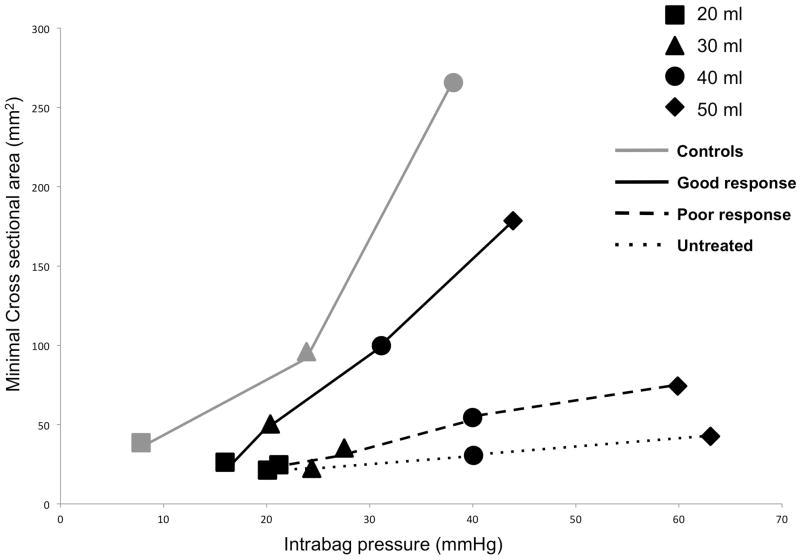
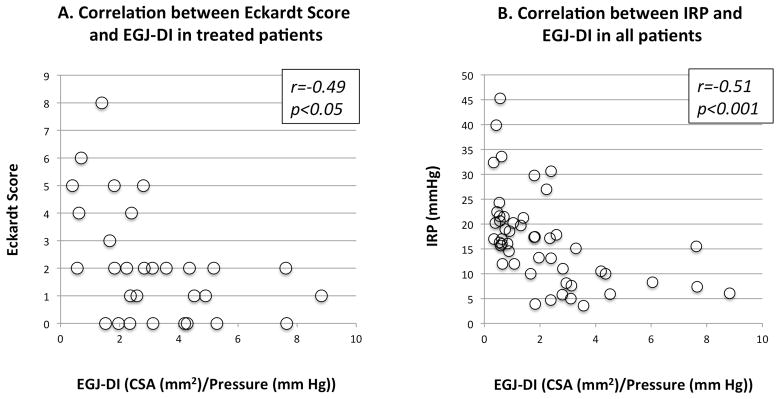
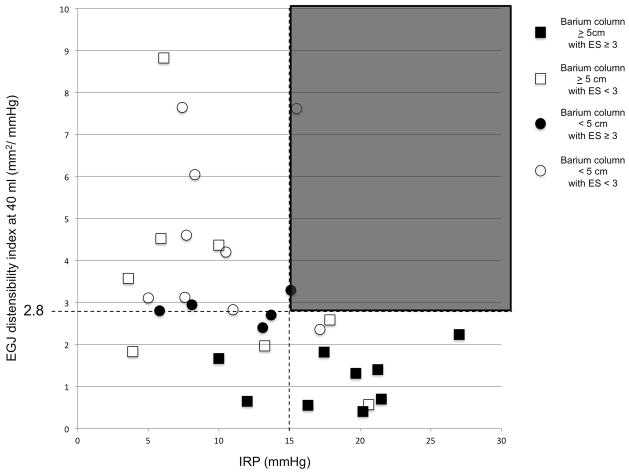
Methods: Findings from FLIP, high-resolution manometry (HRM), timed barium esophagram, and symptom assessment by Eckardt Score (ES) were compared in 54 achalasia patients (23 untreated, 31 treated). Twenty healthy volunteers underwent FLIP as a comparator group. The EGJ distensibility index (EGJ-DI) was defined at the 'waist' of the FLIP bag during volumetric distension, expressed in mm(2) mmHg(-1) . The ES was used to gauge treatment outcome: good response < 3 or poor response ≥ 3.
Key results: Of the 31 treated patients, 17 had good and 14 poor treatment response. The EGJ-DI was significantly different among groups, greatest in the control subjects and least in the untreated patients; patients with good treatment response had significantly greater EGJ-DI than untreated or patients with poor response. The correlations between EGJ-DI and ES and integrated relaxation pressure on HRM were significant.
Conclusions & inferences: The FLIP provided a useful measure of EGJ distensibility in achalasia patients that correlated with symptom severity. The measurement of EGJ distensibility was complementary to existing tests suggesting a potentially important role in the clinical management of achalasia.
© 2013 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Vaezi MF, Baker ME, Richter JE. Assessment of esophageal emptying post-pneumatic dilation: use of the timed barium esophagram. Am J Gastroenterol. 1999;94:1802–1807. - PubMed
-
- Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation. Gastroenterology. 1992;103:1732–1738. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
