

Review
doi: 10.1016/j.clp.2012.12.012.
Epub 2013 Jan 17.
A clinical perspective of necrotizing enterocolitis: past, present, and future
Affiliations
- PMID: 23415262
- PMCID: PMC3575605
- DOI: 10.1016/j.clp.2012.12.012
Item in Clipboard
Review
A clinical perspective of necrotizing enterocolitis: past, present, and future
Clin Perinatol.
2013 Mar.
Abstract
Necrotizing enterocolitis (NEC) primarily affects premature infants. It is less common in term and late preterm infants. The age of onset is inversely related to the postmenstrual age at birth. In term infants, NEC is commonly associated with congenital heart diseases. NEC has also been associated with other anomalies. More than 85% of all NEC cases occur in very low birth weight infants or in very premature infants. Despite incremental advances in our understanding of the clinical presentation and pathophysiology of NEC, universal prevention of this disease continues to elude us even in the twenty-first century.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
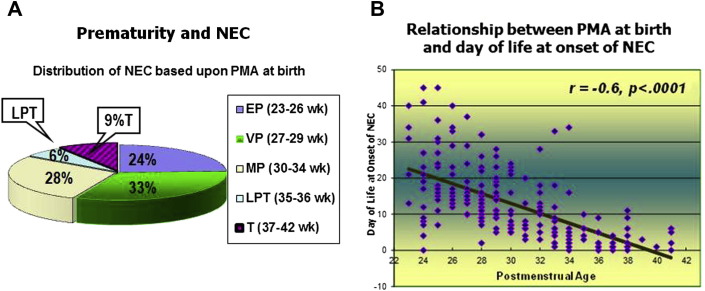
(A) Only 15% of term (T) and late preterm (LPT) infants developed NEC in this cohort of 202 infants with NEC. EP, extremely premature; MP, moderately premature; VP, very premature. (B) Age of onset of NEC is inversely related to PMA at birth.
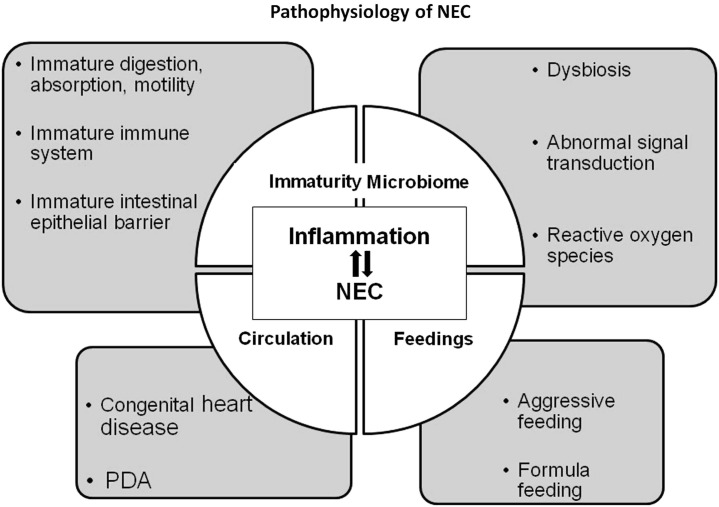
Pathophysiology of NEC.
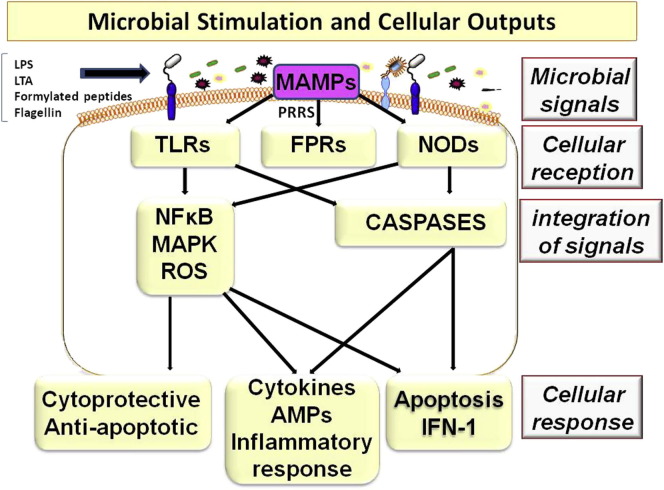
Microbial components, such as lipopolysaccharides (LPS), lipoteichoic acid (LTA), formylated peptides, and flagellin, serve as microbial-associated molecular patterns (MAMPs) and signal pattern recognition receptors (PRRs), including toll-like receptors (TLRs), formylated peptide receptors (FPRs), or nucleotide-binding oligomerization domain-like receptors (NODs). Integration of these signals evokes cellular outputs based on the initial perception of the triggering organism. Output can be a protective response to commensal microbiota, an inflammatory response to pathogenic organisms, or it can trigger apoptosis.
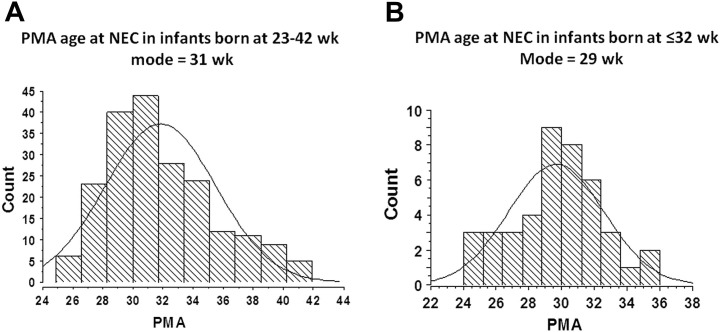
PMA at onset of NEC in 2 different study cohorts. (A) Single-center study cohort of 202 infants with NEC during 1991 to 2003 born at 23 to 42 weeks; NEC was most common at 31 weeks of PMA. (B) Multicenter study cohort of 42 infants with NEC during 2008 to 2012 born at 23 to 32 weeks; NEC occurred most commonly at 29 weeks of PMA.
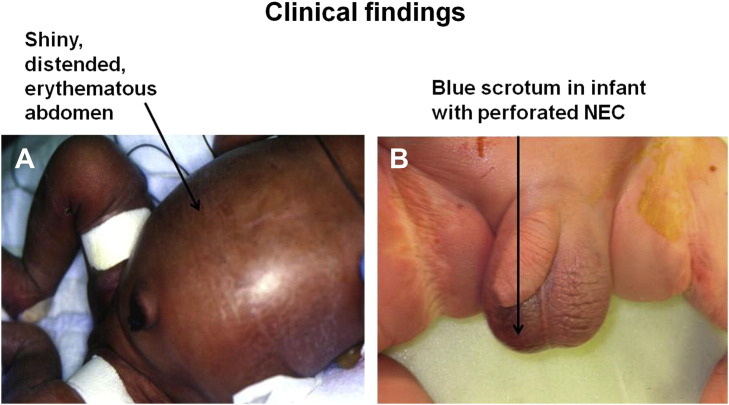
(A) Shiny, distended, erythematous abdomen (arrow) of an infant with advanced NEC in frog-leg position. (B) Discolored scrotum (arrow) in an infant with perforated advanced NEC; no pneumoperitoneum was seen in abdominal radiographs.
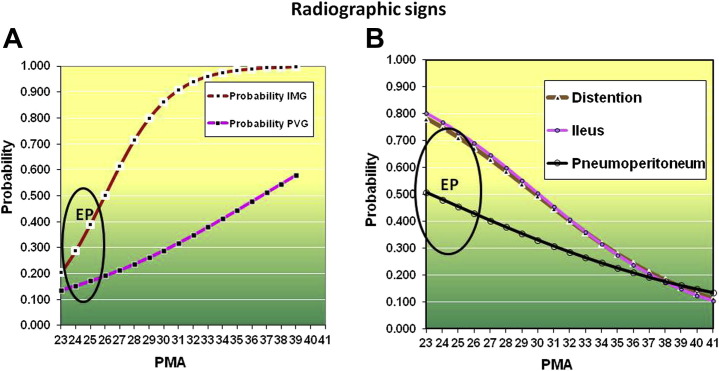
(A) Probability by PMA at birth that an infant with NEC will present with intramural gas (IMG) or portal venous gas (PVG). There is less than 50% probability for an extremely premature (EP) infant to manifest IMG. (B) Radiographic signs that are more probable in infants with decreasing PMA. There is more than 50% probability that an EP infant will present with these signs.
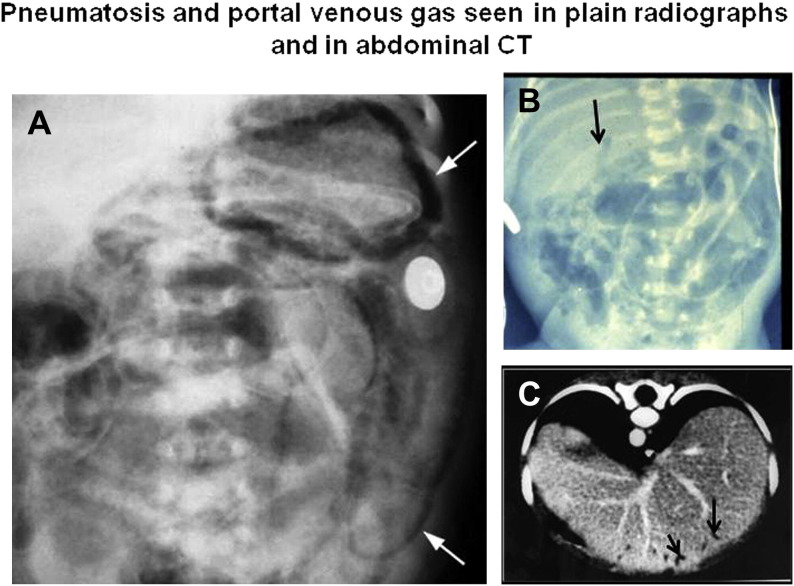
(A) There is extensive pneumatosis (arrows); left upper arrow pointing at gastric pneumatosis. Pneumatosis is seen as multiple curvilinear radiolucencies in this plain radiograph. (B) Arrow pointing toward portal venous gas seen as curvilinear radiolucency over liver; distended bowel loops and diffuse pneumatosis is seen throughout. (C) Portal venous gas (arrows) is seen as lucencies in on computed tomography (CT) scan.
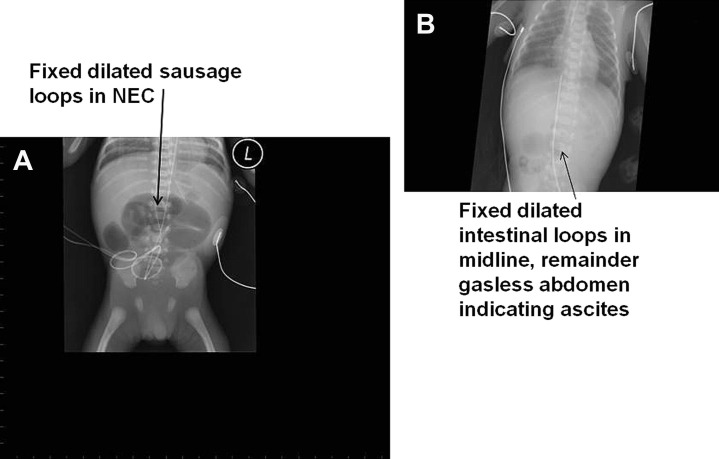
(A) A dynamic loop in serial radiographs indicates intestinal necrosis. (B) Gasless abdomen with a few loops in midline indicates ascites (peritonitis) and intestinal necrosis.
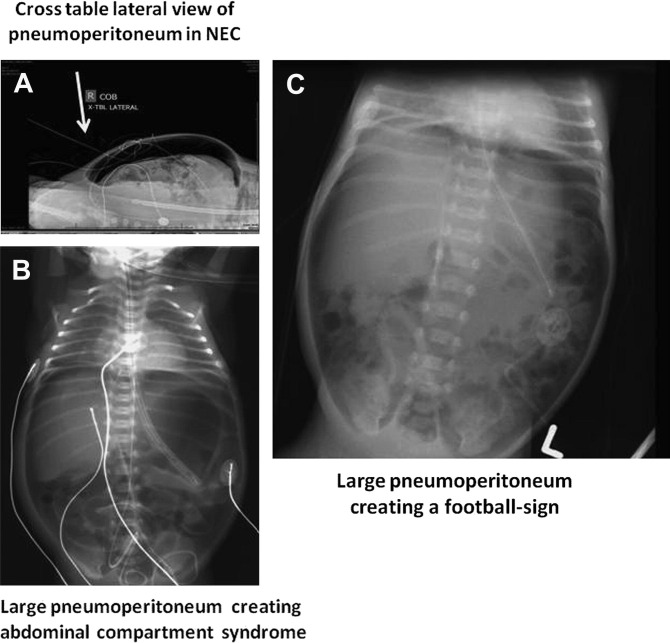
(A) Cross-table lateral and (B) plain abdominal radiographs illustrating radiolucent pneumoperitoneum (indicated by arrows). (C) Another large pneumoperitoneum creating a football sign.
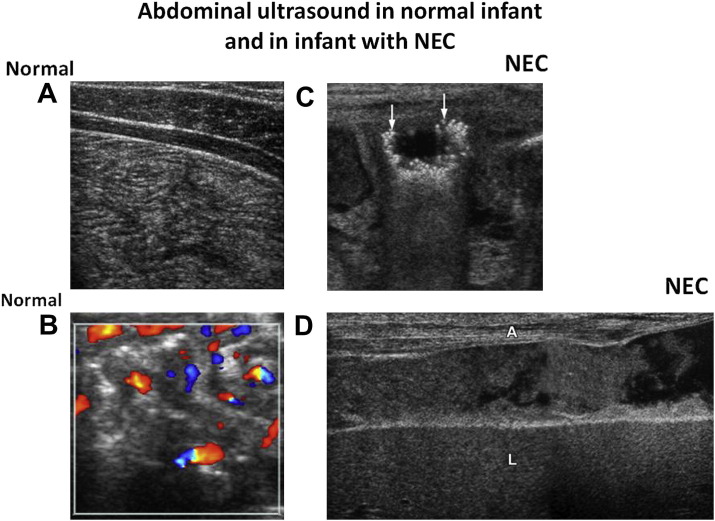
Sonogram of normal bowel (A, B). (A) Normal non-distended bowel; echogenic markings represent mucosal interface with lumen, and hypoechoic linear bands represent the muscularis of the bowel wall. (B) Color Doppler image of non-distended normal bowel with color dots of blood flow in normal bowel. (C) Sonogram shows a distended loop with many pneumatoses seen as hyper-echoic bubbles (arrows). (D) Free intraperitoneal fluid in perforated NEC. Echogenic fluid between abdominal wall (A) and liver (L) is seen containing much debris, which is more indicative of bowel perforation than free fluid.
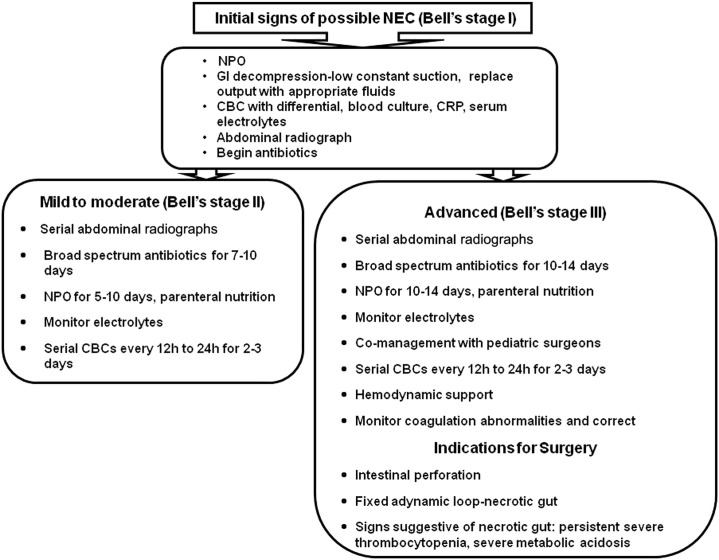
Clinical decision algorithms. NPO, nil per os (nothing by mouth); CBC, complete blood cell count; CRP, C-reactive protein.
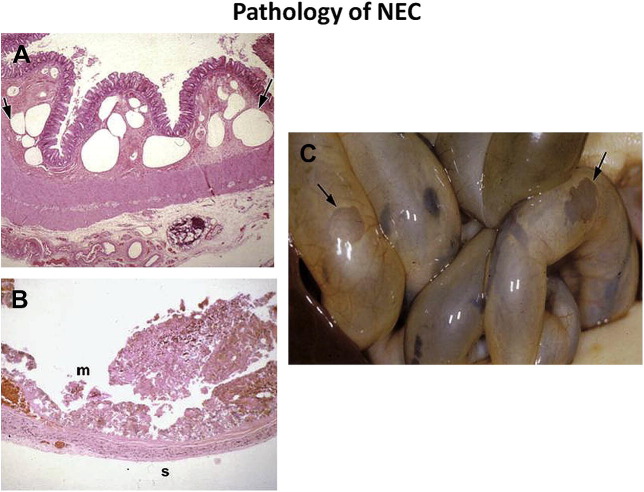
(A) Histology of small bowel (original magnification × 100; hematoxylin-eosin stain) illustrating rounded large bubbles (arrows) of pneumatosis (intramural gas) in the submucosa. (B) At a more advanced stage, there is necrosis of mucosa, submucosa, and muscularis with intraluminal necrotic debris on the mucosal side (m), (original magnification × 100; hematoxylin-eosin stain). Only the serosa (s) appears intact. (C) Gross pathology at postmortem examination shows severe NEC. Arrows indicate severe sloughing of mucosa, submucosa, and muscularis mucosa. Only a thin layer of serosa is intact allowing the intestinal lumen to be seen.
References
-
- Obladen M. Necrotizing enterocolitis –150 years of fruitless search of the cause. Neonatology. 2009;96:203–210. - PubMed
-
- Mizrahi A., Barlow O., Berdon W. Necrotizing enterocolitis in premature infants. J Pediatr. 1965;66:697–705. - PubMed
-
- Touloukian R.J. Neonatal enterocolitis: an update on etiology, diagnosis, and treatment. Surg Clin North Am. 1976;55:376–387. - PubMed
-
- Santulli T.V., Schullinger J.N., Heird W.C. Acute necrotizing enterocolitis in infancy: a review of 64 cases. Pediatrics. 1975;55:376–387. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
