

Risk stratification of ambulatory patients with advanced heart failure undergoing evaluation for heart transplantation
- PMID: 23415315
- PMCID: PMC4119928
- DOI: 10.1016/j.healun.2012.11.026
Risk stratification of ambulatory patients with advanced heart failure undergoing evaluation for heart transplantation
Abstract
Background: Risk stratification of ambulatory heart failure (HF) patients has relied on peak VO(2)<14 ml/kg/min. We investigated whether additional clinical variables might further specify risk of death, ventricular assist device (VAD) implantation (INTERMACS <4) or heart transplantation (HTx, Status 1A or 1B) within 1 year after HTx evaluation. We hypothesized that right ventricular stroke work index (RVSWI), pulmonary capillary wedge pressure (PCWP) and the model for end-stage liver disease-albumin score (MELD-A) would be additive prognostic predictors.
Methods: We retrospectively collected data on 151 ambulatory patients undergoing HTx evaluation. Primary outcomes were defined as HTx, LVAD or death within 1 year after evaluation.
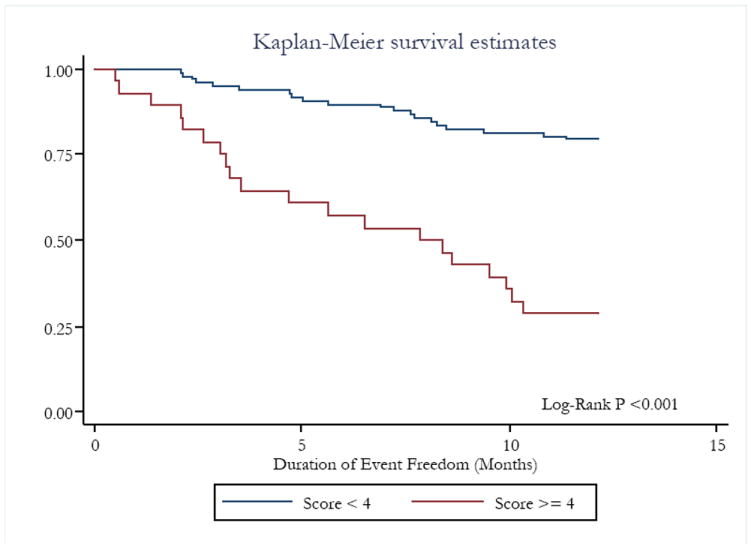
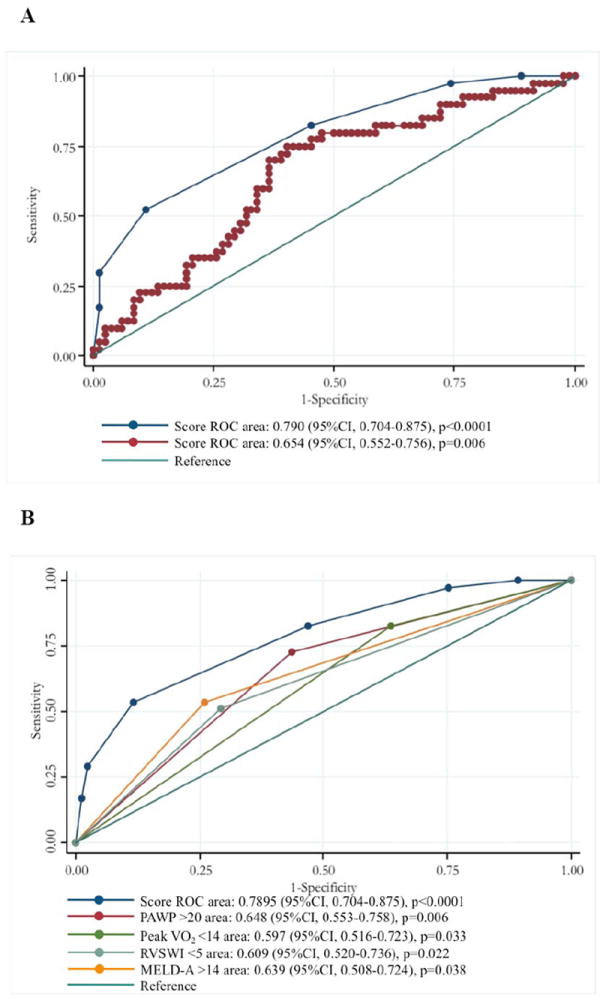
Results: Average age in our cohort was 55 ± 11.1 years, 79.1% were male and 39% had an ischemic etiology (LVEF 21 ± 10.5% and peak VO(2) 12.6 ± 3.5 ml/kg/min). Fifty outcomes (33.1%) were observed (27 HTxs, 15 VADs and 8 deaths). Univariate logistic regression showed a significant association of RVSWI (OR 0.47, p = 0.036), PCWP (OR 2.65, p = 0.007) and MELD-A (OR 2.73, p = 0.006) with 1-year events. Stepwise regression showed an independent correlation of RVSWI<5gm-m(2)/beat (OR 6.70, p < 0.01), PCWP>20 mm Hg (OR 5.48, p < 0.01), MELD-A>14 (OR 3.72, p< 0.01) and peak VO(2)<14 ml/kg/min (OR 3.36, p = 0.024) with 1-year events. A scoring system was developed: MELD-A>14 and peak VO(2)<14-1 point each; and PCWP>20 and RVSWI<5-2 points each. A cut-off at≥4 demonstrated a 54% sensitivity and 88% specificity for 1-year events.
Conclusions: Ambulatory HF patients have significant 1-year event rates. Risk stratification based on exercise performance, left-sided congestion, right ventricular dysfunction and liver congestion allows prediction of 1-year prognosis. Our findings support early and timely referral for VAD and/or transplant.
Copyright © 2013 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Stehlik J, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: Twenty-eighth Adult Heart Transplant Report—2011. J Heart Lung Transplant. 2011;30:1078–94. - PubMed
-
- Jaski BE, Kim JC, Naftel DC, et al. Cardiac Transplant Research Database Research Group. Cardiac transplant outcome of patients supported on left ventricular assist device vs. intravenous inotropic therapy. J Heart and Lung Transplant. 2001;20:449–56. - PubMed
-
- Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation. 1997;95:2660–7. - PubMed
-
- Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424–1433. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH, Jr, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83:778–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
