

Procalcitonin levels to guide antibiotic therapy in adults with non-microbiologically proven apparent severe sepsis: a randomised controlled trial
- PMID: 23418298
- PMCID: PMC3586059
- DOI: 10.1136/bmjopen-2012-002186
Procalcitonin levels to guide antibiotic therapy in adults with non-microbiologically proven apparent severe sepsis: a randomised controlled trial
Abstract
Objective: Some patients with the phenotype of severe sepsis may have no overt source of infection or identified pathogen. We investigated whether a procalcitonin-based algorithm influenced antibiotic use in patients with non-microbiologically proven apparent severe sepsis.
Design: This multicentre, randomised, controlled, single-blind trial was performed in two parallel groups.
Setting: Eight intensive care units in France.
Participants: Adults with the phenotype of severe sepsis and no overt source of infection, negative microbial cultures from multiple matrices and no antibiotic exposure shortly before intensive care unit admission.
Intervention: The initiation and duration of antibiotic therapy was based on procalcitonin levels in the experimental arm and on the intensive care unit physicians' clinical judgement without reference to procalcitonin values in the control arm.
Main outcome measure: The primary outcome was the proportion of patients on antibiotics on day 5 postrandomisation.
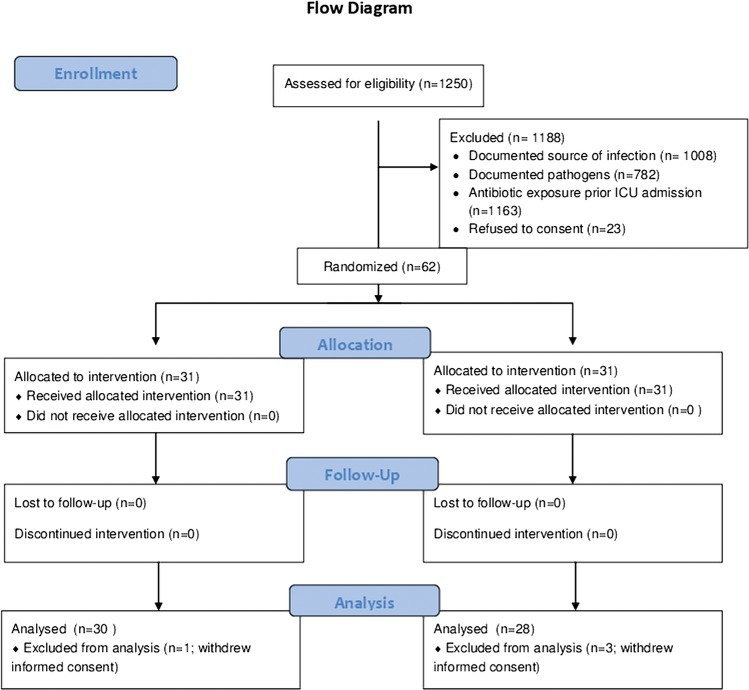
Results: Over a 3-year period, 62/1250 screened patients were eligible for the study, of whom 31 were randomised to each arm; 4 later withdrew their consent. At day 5, 18/27 (67%) survivors were on antibiotics in the experimental arm, versus 21/26 (81%) controls (p=0.24; relative risk=0.83, 95% CI: 0.60 to 1.14). Only 8/58 patients (13%) had baseline procalcitonin <0.25 µg/l; in these patients, physician complied poorly with the algorithm.
Conclusions: In intensive care unit patients with the phenotype of severe sepsis or septic shock and without an overt source of infection or a known pathogen, the current study was unable to confirm that a procalcitonin-based algorithm may influence antibiotic exposure. However, the premature termination of the trial may not allow definitive conclusions.
References
-
- Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet 2005;365:63–78 - PubMed
-
- Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009;302:2323–9 - PubMed
-
- Annane D, Vignon P, Renault A, et al. Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomized trial. Lancet 2007;370:676–84 - PubMed
-
- Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med 2008;358:111–24 - PubMed
-
- Russell JA, Walley KR, Singer J, et al. Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med 2008;358:877–87 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical