

Lanthanum carbonate versus placebo for management of hyperphosphatemia in patients undergoing peritoneal dialysis: a subgroup analysis of a phase 2 randomized controlled study of dialysis patients
- PMID: 23418668
- PMCID: PMC3582545
- DOI: 10.1186/1471-2369-14-40
Lanthanum carbonate versus placebo for management of hyperphosphatemia in patients undergoing peritoneal dialysis: a subgroup analysis of a phase 2 randomized controlled study of dialysis patients
Abstract
Background: This short-term study assessed the efficacy and safety of lanthanum carbonate in the treatment of hyperphosphatemia in dialysis patients; here, we report a prespecified subgroup analysis of patients undergoing peritoneal dialysis.
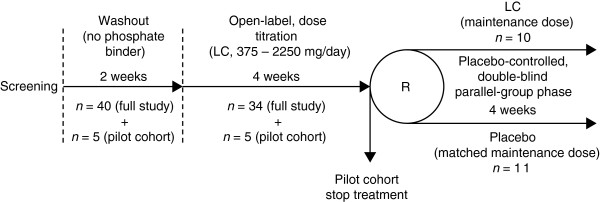
Methods: Men and women (n=39) who had received continuous ambulatory peritoneal dialysis for chronic kidney disease for 6 months or more were enrolled in eight renal medicine departments in the United Kingdom. A 2-week washout period was followed by a 4-week dose-titration phase during which patients received lanthanum carbonate titrated up to 2250 mg/day. This was followed by a 4-week, randomized, placebo-controlled, parallel-group phase during which patients continued to receive either lanthanum carbonate at the titrated dose, or a matched dose of placebo. The main outcome measure was control of serum phosphate levels (1.3-1.8 mmol/l) at the end of the parallel-group phase.
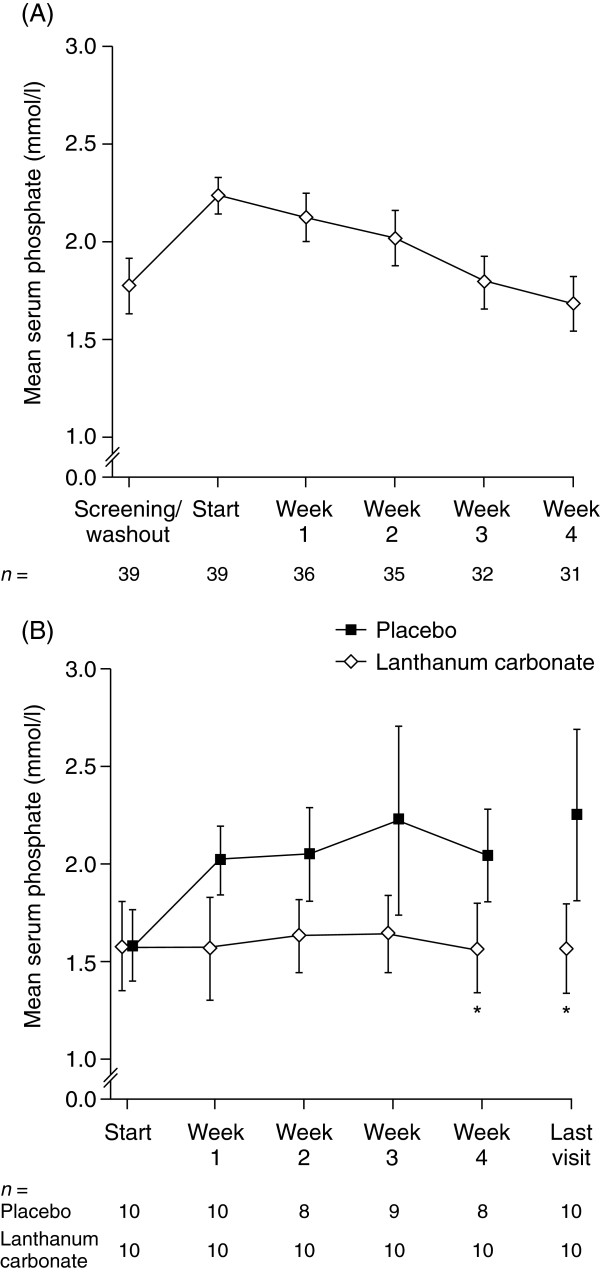
Results: Serum phosphate was controlled in 3/39 (8%) patients at the beginning of the dose-titration phase (after washout) and in 18/31 (58%) patients treated with lanthanum carbonate at its end. After the parallel-group phase, 60% of lanthanum carbonate-treated patients and 10% of those receiving placebo had controlled serum phosphate. There was no difference in mean (95% confidence interval) serum phosphate levels between groups at randomization: lanthanum carbonate, 1.57 (1.34-1.81) mmol/l; placebo, 1.58 (1.40-1.76) mmol/l (p=0.96). However, a difference was seen at the end of the parallel-group phase: lanthanum carbonate, 1.56 (1.33-1.79) mmol/l; placebo, 2.25 (1.81-2.68) mmol/l (p=0.0015). There were no clinically important changes in nutritional parameters and no serious treatment-related adverse events were recorded.
Conclusions: At doses up to 2250 mg/day, lanthanum carbonate is well tolerated and controls hyperphosphatemia effectively. Treatment with higher doses of lanthanum carbonate may allow patients undergoing peritoneal dialysis the potential to increase their dietary protein intake without compromising their phosphate control.
Figures
References
-
- Eknoyan G, Levin A, Levin N. National kidney foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis. 2003;42(Suppl 3):S1–S201. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
