

Update on the targeted therapy of melanoma
- PMID: 23420410
- PMCID: PMC6684217
- DOI: 10.1007/s11864-013-0226-8
Update on the targeted therapy of melanoma
Abstract
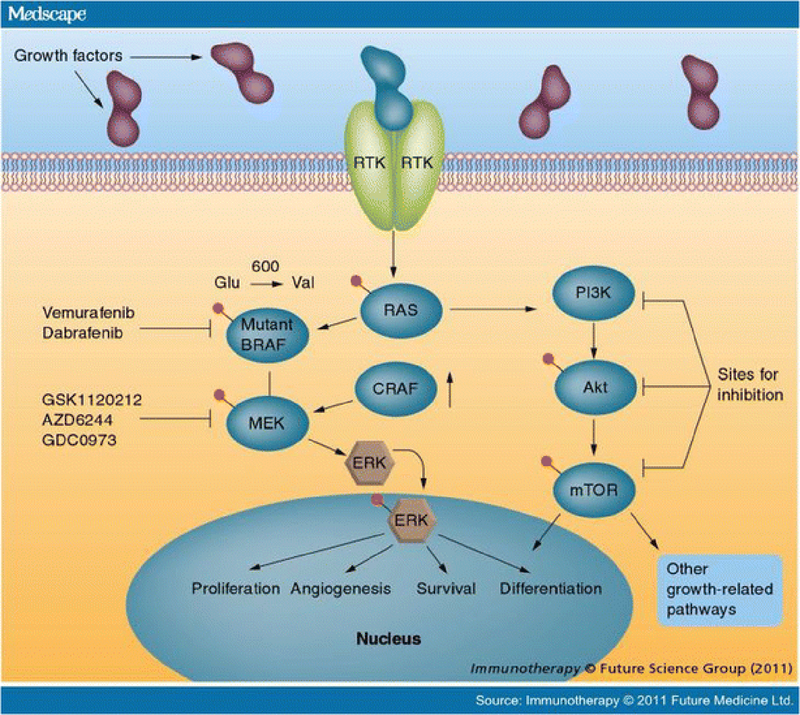
Melanoma is the most aggressive of the cutaneous malignancies, causing more than 9,000 deaths in the past year in the United States. Historically, systemic therapies have been largely ineffective, because melanoma is usually resistant to cytotoxic chemotherapy. However, during the past few years, several targeted therapies have proved effective in this challenging disease. These recent advances have been facilitated by an improved understanding of the driving genetic aberrations of melanoma, particularly mutations in the mitogen-activated protein kinase (MAPK) pathway. Vemurafenib, a BRAF inhibitor, demonstrated an overall survival advantage in phase III trials and is an appropriate option for first-line therapy in metastatic BRAF mutant melanoma. Dabrafenib, another BRAF inhibitor, and trametinib, a MEK inhibitor, also have been shown to be effective in phase III trials for BRAF mutant melanoma and may be additional treatment options as monotherapy or in combination pending regulatory approval. Additionally, imatinib is a promising targeted therapy for patients whose tumors harbor a KIT mutation in exons 11 and 13. Although these targeted agents cause objective responses and clinical benefit in patients with metastatic melanoma, resistance invariably develops. New targets and strategies to overcome acquired resistance are urgently needed. Furthermore, no effective targeted therapy has been developed for NRAS mutant tumors or in melanomas with as yet unknown driver mutations. In this review, we discuss current molecular targeted treatment options and promising ongoing research to develop new strategies to treat melanoma.
Figures
References
-
- American Cancer Society Cancer Facts and Figures 2012, 2012, American Cancer Society: Atlanta.
-
- Jemal A, Saraiya M, Patel P, et al., Recent trends in cutaneous melanoma incidence and death rates in the United States, 1992–2006. J Am Acad Dermatol, 2011, 65:S17–25 e1–3. - PubMed
-
This study highlights the epidemiology and mortality trends in melanoma.
-
- Long GV, Menzies AM, Nagrial AM, et al., Prognostic and clinicopathologic associations of oncogenic BRAF in metastatic melanoma. J Clin Oncol, 2011, 29:1239–46. - PubMed
-
- Beadling C, Jacobson-Dunlop E, Hodi FS, et al., KIT gene mutations and copy number in melanoma subtypes. Clin Cancer Res, 2008, 14:6821–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
