

Biomarkers for the clinical evaluation of the cognitively impaired elderly: amyloid is not enough
- PMID: 23420460
- PMCID: PMC3573528
- DOI: 10.2217/iim.12.27
Biomarkers for the clinical evaluation of the cognitively impaired elderly: amyloid is not enough
Abstract
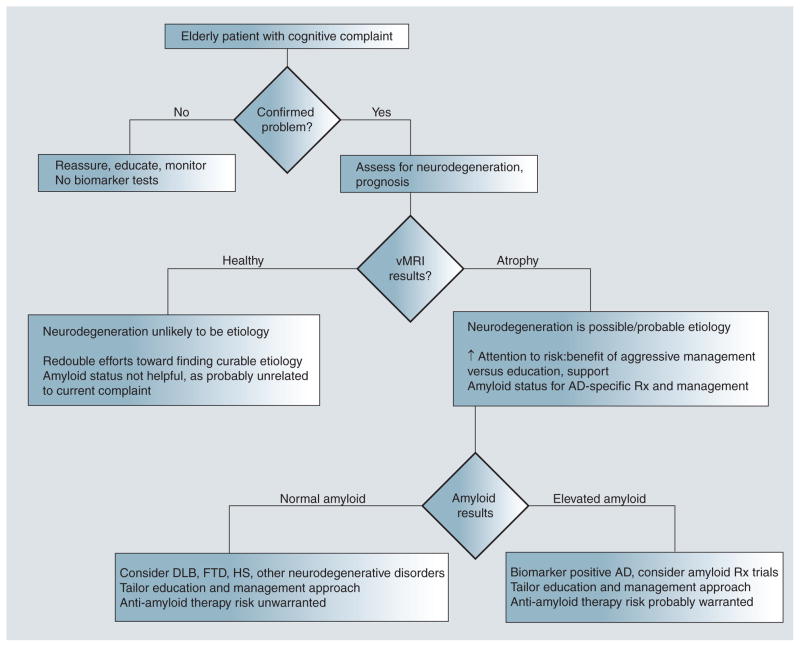
The number of elderly patients seeking clinical treatment for memory problems will rise sharply in coming years as our population ages. These patients present a challenge for diagnosis and prognosis since cognitive problems in older patients can arise from many etiologies, some of which are curable. With the development of clinically available biomarkers for detecting Alzheimer's disease pathology in living patients, evaluation of cognitively impaired elderly patients is about to undergo a major paradigm shift. This article describes the two classes of biomarkers available for assessing Alzheimer's disease risk: those that indicate presence of amyloid pathology and those that provide evidence of neuronal injury and neurodegeneration. We argue that, currently, incorporation of biomarkers of neurodegeneration can help in patient prognosis whereas tests for amyloid, if used in isolation, have potential for harm. Amyloid tests are clinically useful only when evidence suggests progressive cognitive decline or neurodegeneration.
Keywords: Alzheimer’s disease; MCI; MRI; PET; amyloid imaging; biomarker; florbetapir; mild cognitive impairment.
Figures
References
-
- Klunk WE, Engler H, Nordberg A, et al. Imaging brain amyloid in Alzheimer’s disease with Pittsburgh compound-B. Ann Neurol. 2004;55(3):306–319. First study to report imaging of amyloid in the living human brain. - PubMed
-
- Rowe CC, Ackerman U, Browne W, et al. Imaging of amyloid β in Alzheimer’s disease with 18F-BAY94–9172, a novel PET tracer: proof of mechanism. Lancet Neurol. 2008;7(2):129–135. - PubMed
-
- Herholz K, Ebmeier K. Clinical amyloid imaging in Alzheimer’s disease. Lancet Neurol. 2011;10(7):667–670. - PubMed
-
- Department of Economic and Social Affairs. World population ageing. United Nations Publications; UN, NY, USA: 2001. Population Division.
Website
-
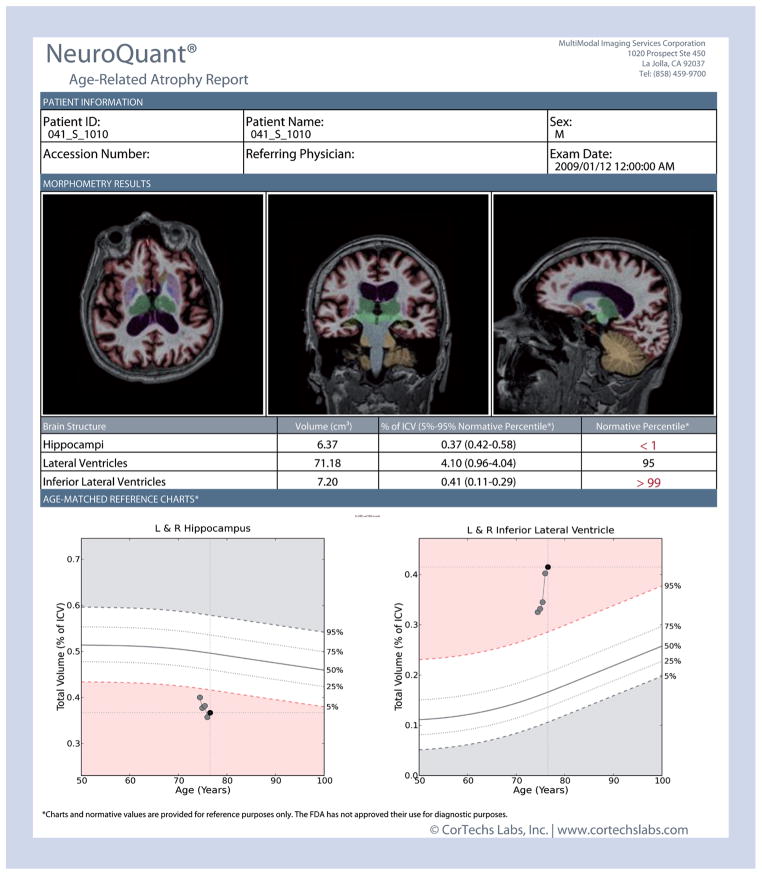
- NeuroQuant®. www.cortechslabs.com.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources