

Estimating the glomerular filtration rate from serum creatinine is better than from cystatin C for evaluating risk factors associated with chronic kidney disease
- PMID: 23423253
- PMCID: PMC3661736
- DOI: 10.1038/ki.2013.7
Estimating the glomerular filtration rate from serum creatinine is better than from cystatin C for evaluating risk factors associated with chronic kidney disease
Erratum in
- Kidney Int. 2013 Aug;84(2):419
Abstract
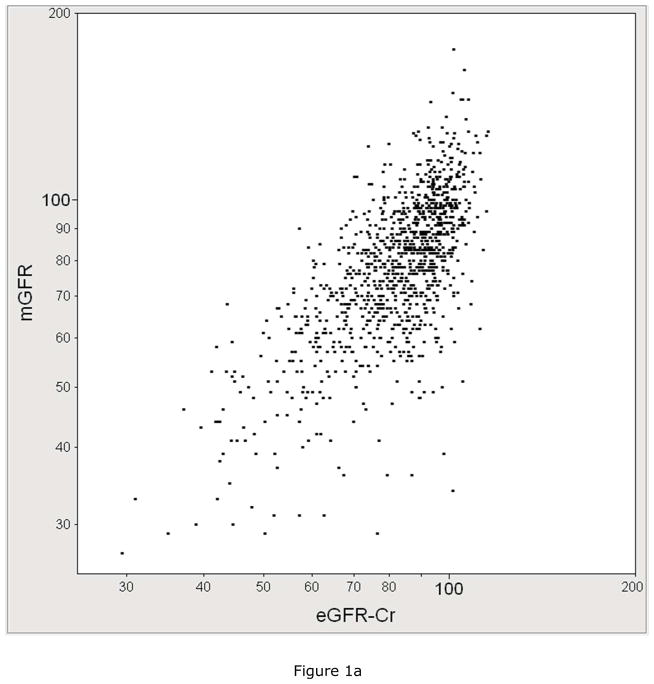
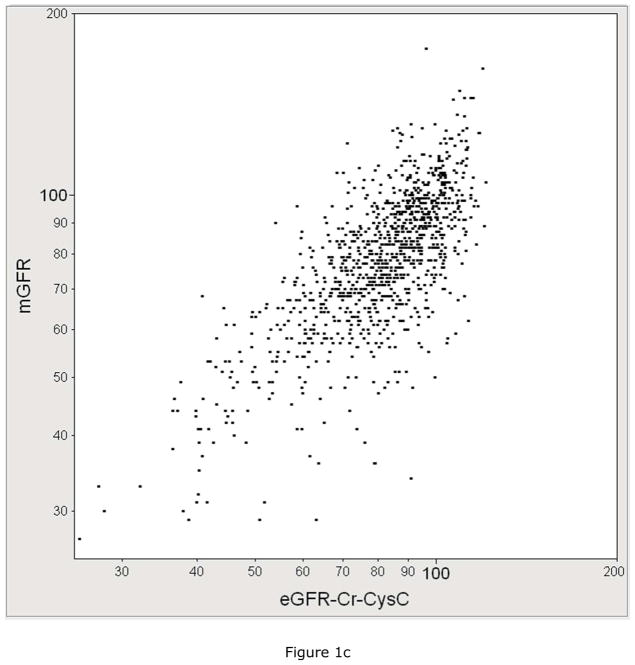
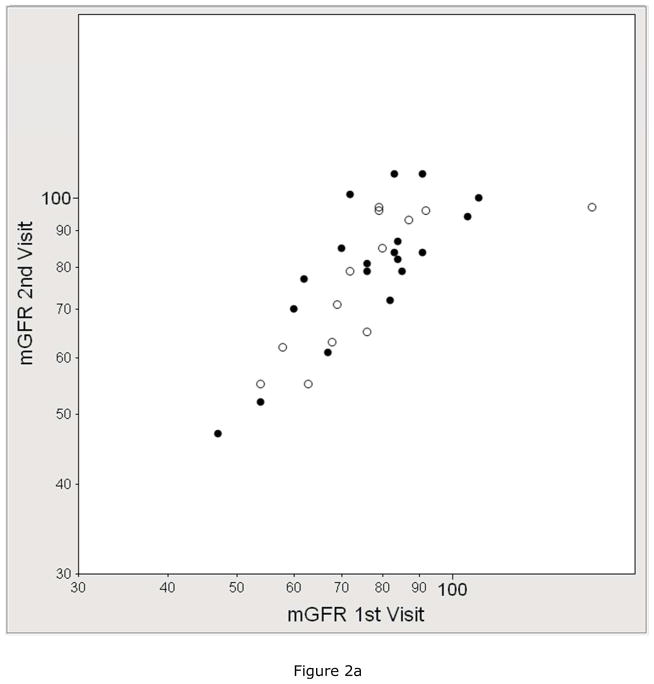
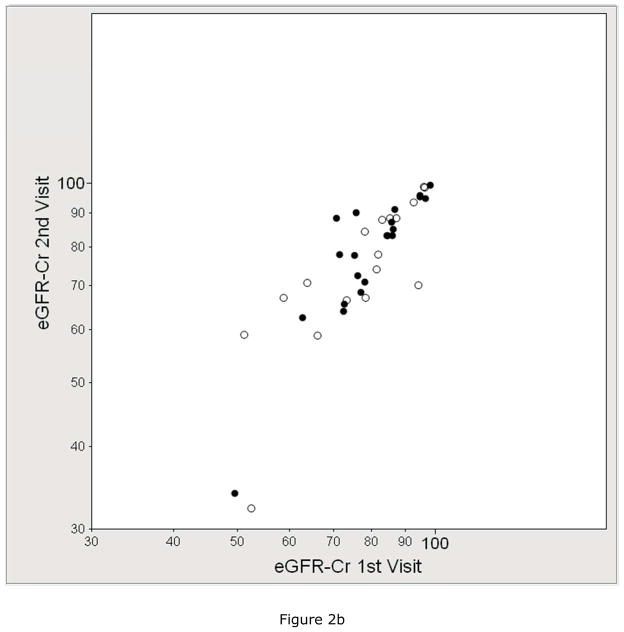
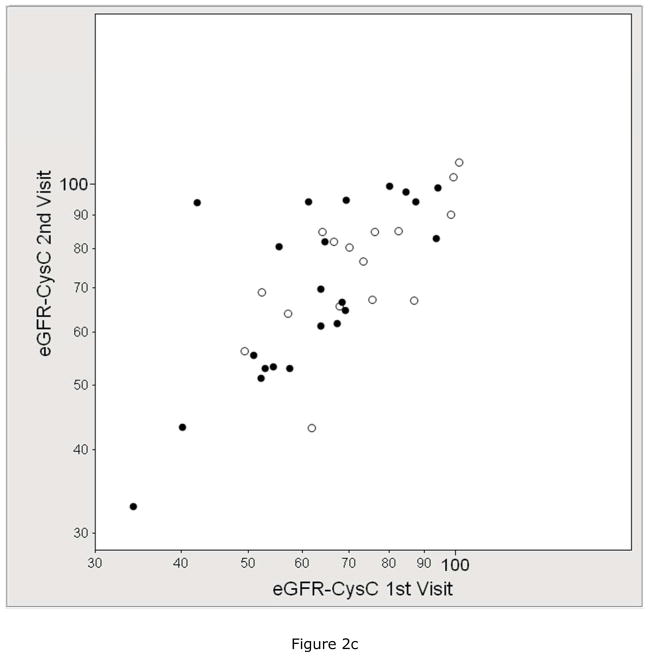
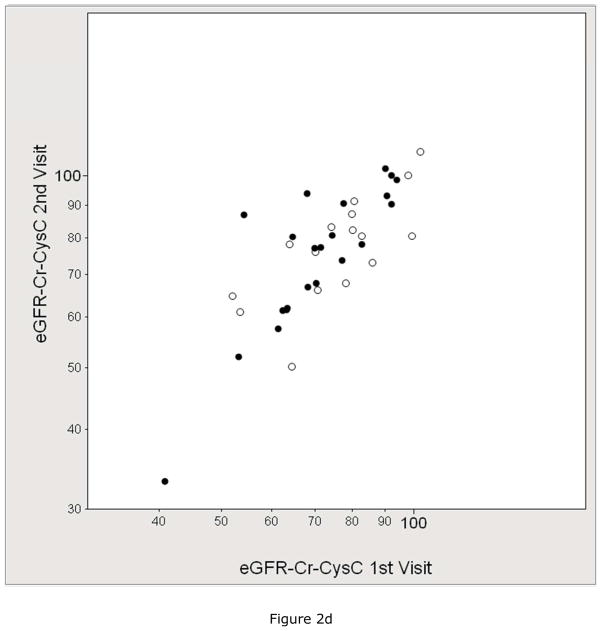
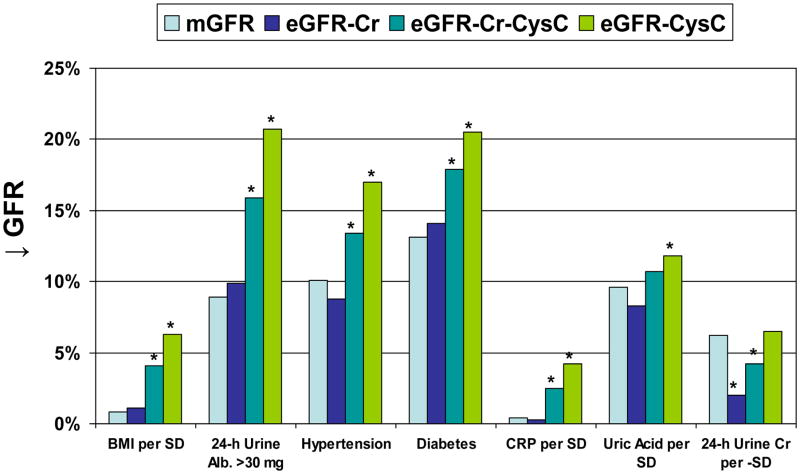
Chronic kidney disease risk factors may associate with the estimated glomerular filtration rate (eGFR) differently than with the measured GFR. To examine this, we evaluated 1150 patients (mean age 65 years) in two community cohorts for risk factors, measured GFR by iothalamate clearance, and eGFR based on creatinine (Cr), cystatin C (CysC), or both. The interaction between each risk factor and eGFR (relative to measured GFR) identified risk factor associations with eGFR along non-GFR pathways. In a subset of 40 patients with two visits, the mean coefficient of variation was 8.2% for measured GFR, 6.4% for eGFRCr, 8.2% for eGFRCr-CysC, and 10.7% for eGFRCysC. The measured GFR was better correlated with eGFRCr-CysC (r, 0.74) than eGFRCr (r, 0.70) or eGFRCysC (r, 0.68). Lower measured GFR associated with lower 24-hour urine creatinine, albuminuria, hypertension, diabetes, higher triglycerides, and higher uric acid. Lower eGFRCr had these same associations except for an association with higher 24-hour urine creatinine along a non-GFR pathway. Lower eGFRCysC and eGFRCr-CysC also had these same associations but also associated with obesity, albuminuria, hypertension, diabetes, higher triglycerides, higher C-reactive protein, and higher uric acid along non-GFR pathways. Thus, cystatin C improves estimation of GFR over creatinine alone; however, the association between most of the risk factors and GFR was more accurate by eGFR based on creatinine alone. This is explained by the association of these risk factors with the non-GFR determinants of cystatin C.
Conflict of interest statement
Figures

Comment in
-
Chronic kidney disease: Cystatin-C-based eGFR: what is it telling us?Nat Rev Nephrol. 2013 Jun;9(6):318-9. doi: 10.1038/nrneph.2013.77. Epub 2013 Apr 16. Nat Rev Nephrol. 2013. PMID: 23591444 No abstract available.
References
-
- Menon V, Shlipak MG, Wang X, et al. Cystatin C as a risk factor for outcomes in chronic kidney disease. Annals of Internal Medicine. 2007;147:19–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
