

Femoroacetabular impingement predisposes to traumatic posterior hip dislocation
- PMID: 23423625
- PMCID: PMC3706669
- DOI: 10.1007/s11999-013-2863-4
Femoroacetabular impingement predisposes to traumatic posterior hip dislocation
Abstract
Background: Traumatic posterior hip dislocation in adults is generally understood to be the result of a high-energy trauma. Aside from reduced femoral antetorsion, morphologic risk factors for dislocation are unknown. We previously noticed that some hips with traumatic posterior dislocations had evidence of morphologic features of femoroacetabular impingement (FAI), therefore, we sought to evaluate that possibility more formally.
Questions/purposes: We asked whether hips with a traumatic posterior hip dislocation present with (1) a cam-type deformity and/or (2) a retroverted acetabulum.
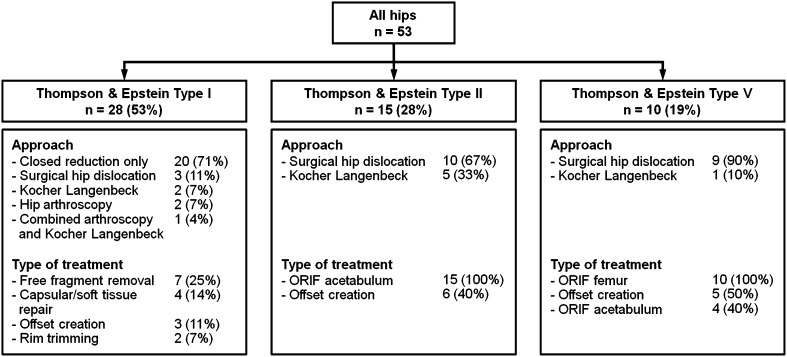
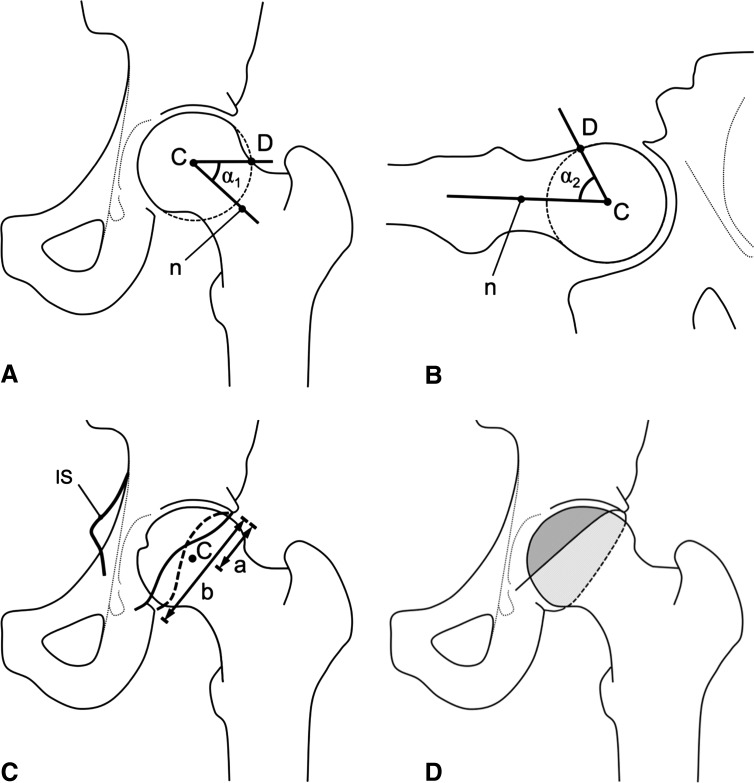
Methods: We retrospectively compared the morphologic features of 53 consecutive hips (53 patients) after traumatic posterior hip dislocation with 85 normal hips (44 patients) based on AP pelvic and crosstable axial radiographs. We measured the axial and the lateral alpha angle for detection of a cam deformity and the crossover sign, ischial spine sign, posterior wall sign, retroversion index, and ratio of anterior to posterior acetabular coverage to describe the acetabular orientation.
Results: Hips with traumatic posterior traumatic dislocation were more likely to have cam deformities than were normal hips, in that the hips with dislocation had increased axial and lateral alpha angles. Hips with posterior dislocation also were more likely to be retroverted; dislocated hips had a higher prevalence of a positive crossover sign, ischial spine sign, and posterior wall sign, and they had a higher retroversion index and increased ratio of anterior to posterior acetabular coverage.
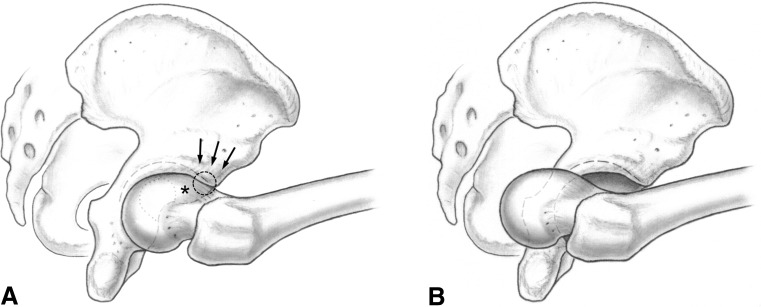
Conclusions: Hips with posterior traumatic dislocation typically present with morphologic features of anterior FAI, including a cam-type deformity and retroverted acetabulum. An explanation for these findings could be that the early interaction between the aspherical femoral head and the prominent acetabular rim acts as a fulcrum, perhaps making these hips more susceptible to traumatic dislocation.
Figures

Comment in
-
CORR Insights™: Femoroacetabular impingement predisposes to traumatic posterior hip dislocation.Clin Orthop Relat Res. 2013 Jun;471(6):1944-5. doi: 10.1007/s11999-013-2910-1. Epub 2013 Mar 8. Clin Orthop Relat Res. 2013. PMID: 23471554 Free PMC article. No abstract available.
-
Reply to the Letter to the editor: Femoroacetabular impingement predisposes to traumatic posterior hip dislocation.Clin Orthop Relat Res. 2013 Nov;471(11):3720-1. doi: 10.1007/s11999-013-3276-0. Epub 2013 Sep 7. Clin Orthop Relat Res. 2013. PMID: 24014272 Free PMC article. No abstract available.
-
Letter to the editor: Femoroacetabular impingement predisposes to traumatic posterior hip dislocation.Clin Orthop Relat Res. 2013 Nov;471(11):3718-9. doi: 10.1007/s11999-013-3275-1. Epub 2013 Sep 13. Clin Orthop Relat Res. 2013. PMID: 24030625 Free PMC article. No abstract available.
References
-
- Dreinhofer KE, Schwarzkopf SR, Haas NP, Tscherne H. Isolated traumatic dislocation of the hip: long-term results in 50 patients. J Bone Joint Surg Br. 1994;76:6–12. - PubMed
-
- Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
