

Type 2 diabetes with partial lipodystrophy of the limbs: a new lipodystrophy phenotype
- PMID: 23423695
- PMCID: PMC3714521
- DOI: 10.2337/dc12-1529
Type 2 diabetes with partial lipodystrophy of the limbs: a new lipodystrophy phenotype
Abstract
Objective: Lipodystrophies are categorized by the extent of fat loss (generalized vs. partial) and by inheritance (congenital vs. acquired). We examined whether a group of patients with partial lipodystrophy of the limbs (PLL), type 2 diabetes mellitus (T2DM), and an absence of a family history of lipodystrophy constitute a new clinical subtype.
Research design and methods: Ten women with T2DM and PLL were identified in academic diabetes clinics and were matched by age, sex, BMI, ethnicity, and diabetes status with 10 women with control T2DM without lipodystrophy. All patients were characterized by clinical evaluation and hyperinsulinemic clamp.
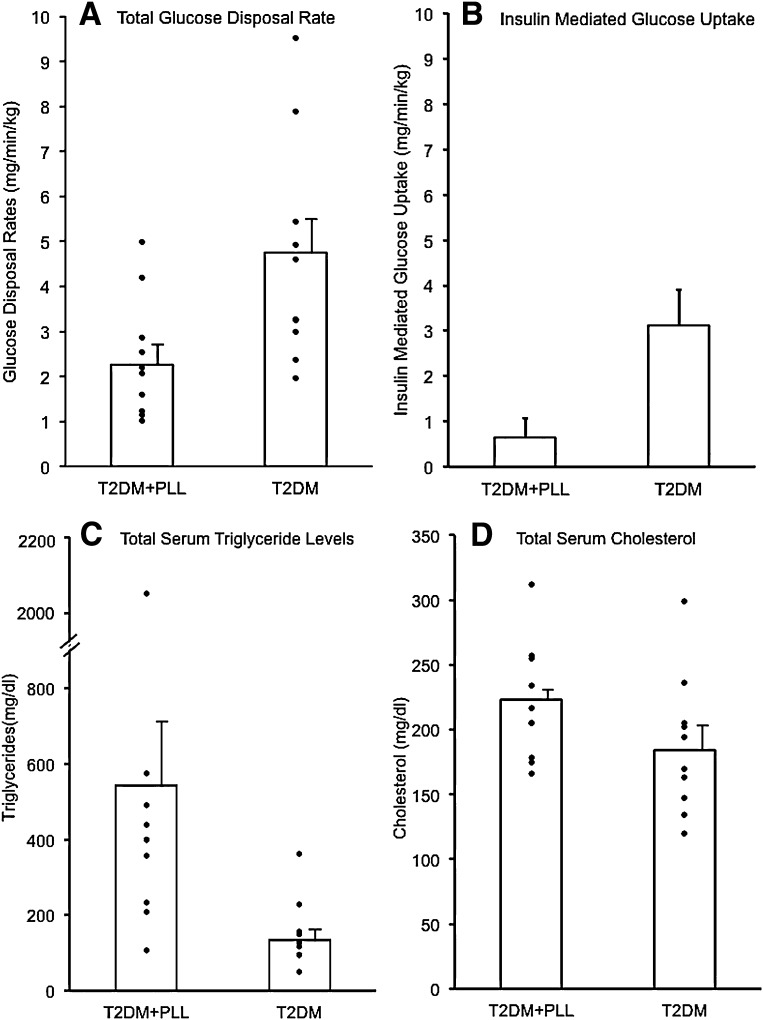
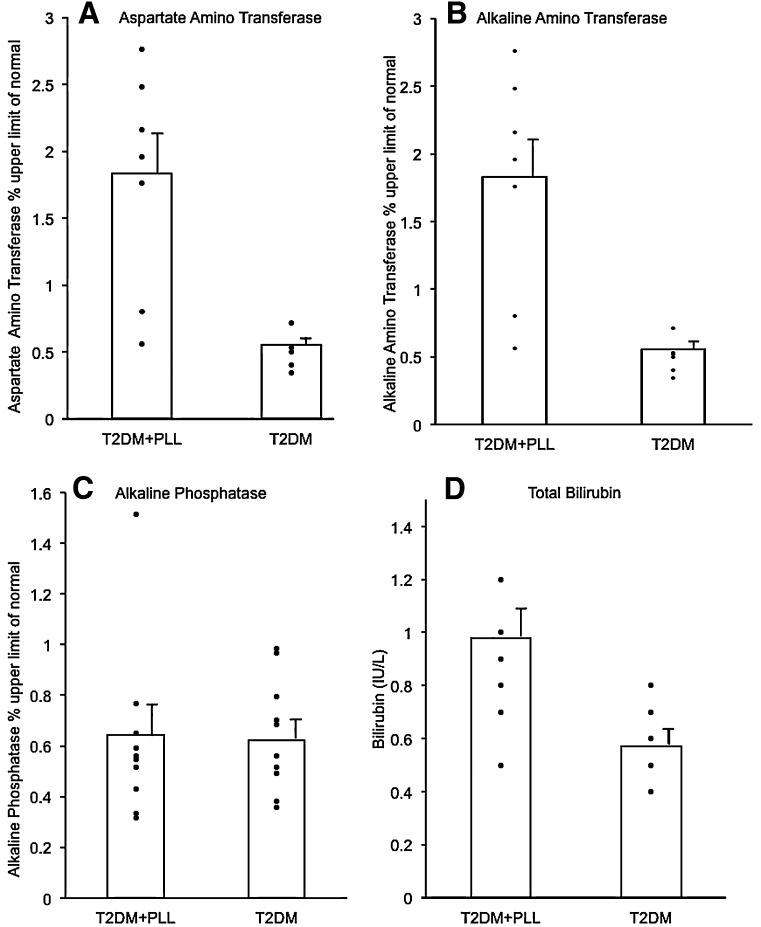
Results: Patients with T2DM and PLL exhibited symmetrical loss of subcutaneous fat in forearms, or forearms plus calves, and acanthosis nigricans. Maximally stimulated glucose disposal rates were markedly reduced by 56% in the T2DM with PLL group compared with the control T2DM patients, whether normalized by body weight or surface area. Most PLL patients exhibited little or no insulin-mediated glucose uptake after subtraction of non-insulin-mediated glucose uptake. The T2DM with PLL group also had greater elevations in hepatic transaminases and triglycerides and earlier onset of diabetes compared with control T2DM.
Conclusions: T2DM with PLL represents a previously unrecognized phenotype of lipodystrophy and of T2DM. These T2DM patients exhibit symmetrical lipodystrophy of the distal limbs, acanthosis nigricans, marked insulin resistance with little insulin-mediated glucose uptake, hypertriglyceridemia, and hepatic transaminase elevations, which are greater in severity than observed in patients with common T2DM.
Figures

Comment in
-
Novel forms of lipodystrophy: why should we care?Diabetes Care. 2013 Aug;36(8):2142-5. doi: 10.2337/dc13-0561. Diabetes Care. 2013. PMID: 23881965 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
