

Review
doi: 10.1161/CIRCGENETICS.110.959387.
A clinical approach to inherited hypertrophy: the use of family history in diagnosis, risk assessment, and management
Affiliations
- PMID: 23424256
- PMCID: PMC3898734
- DOI: 10.1161/CIRCGENETICS.110.959387
Item in Clipboard
Review
A clinical approach to inherited hypertrophy: the use of family history in diagnosis, risk assessment, and management
Circ Cardiovasc Genet.
2013 Feb.
No abstract available
Figures
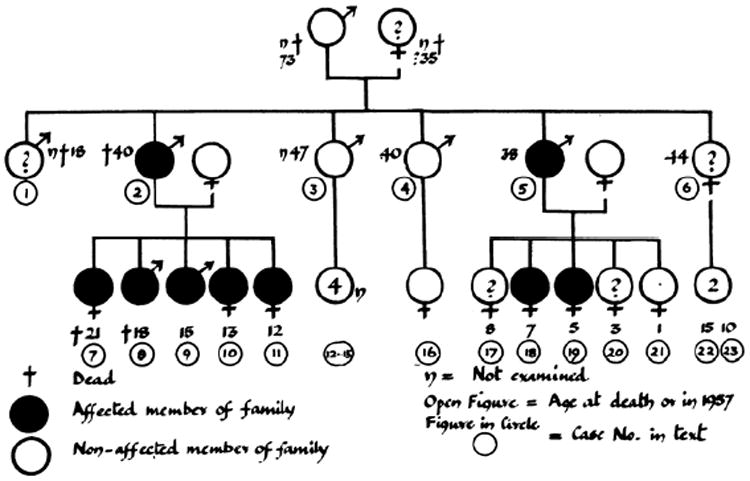
Published in 1960, this family pedigree was the first to show autosomal dominant inheritance of hypertrophic cardiomyopathy (HCM). Females are represented by the symbol for Venus (♀), males by the symbol for Mars (♂). Filled shapes indicate verified disease. Adapted with permission from Hollman et al.
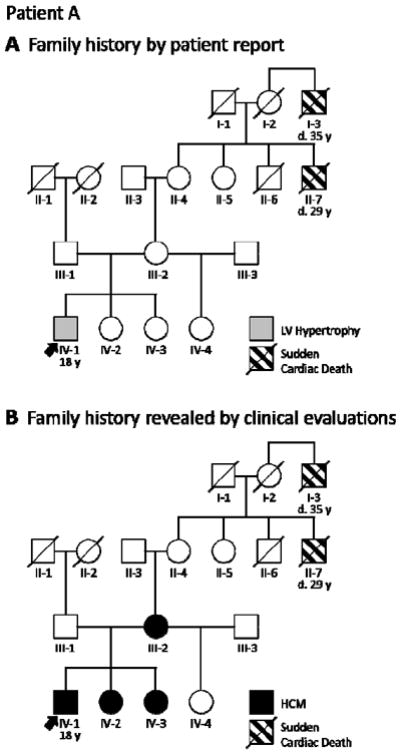
Strategic clinical assessment of a patient’s close family members aids diagnosis by adding valuable information to the family history. A, When 18-year-old Patient A (arrow) presented with mild left ventricular (LV) hypertrophy, his family history of sudden cardiac death (I-3 and II-7) raised suspicion for HCM. B, Clinical cardiology evaluation of the patient’s mother (III-2) and sisters (IV-2 and IV-3) provided the evidence needed for diagnosis. Circles indicate females; squares, males; slash, deceased. HCM = hypertrophic cardiomyopathy.
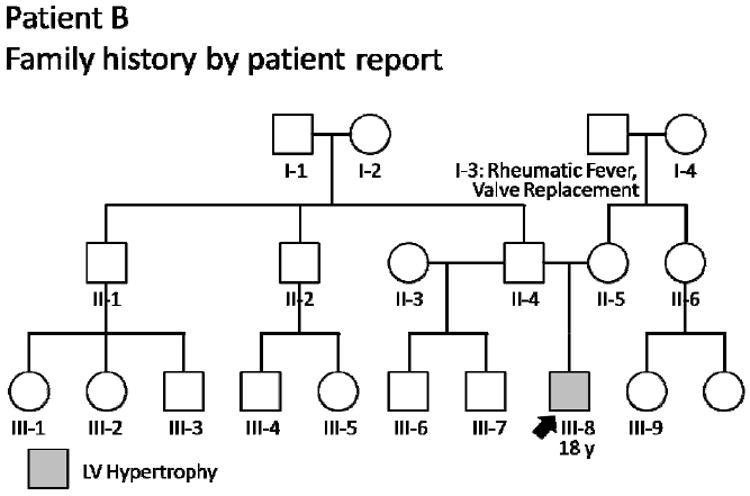
An uneventful family history lowers suspicion for HCM, prompting more thorough investigation of alternative etiologies. For 18-year-old Patient B (arrow) with mild left ventricular (LV) hypertrophy, 24-hour blood pressure monitoring revealed occult hypertension as the underlying cause. Circles indicate females; squares, males; slash, deceased. HCM = hypertrophic cardiomyopathy.
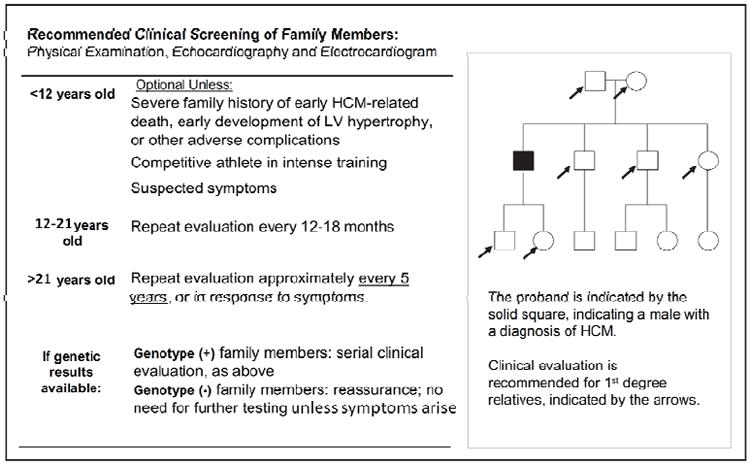
Screening recommendations for families with HCM. The frequency of screening is based on the age of the at-risk family member, due to the age-dependent penetrance of left ventricular (LV) hypertrophy. HCM = hypertrophic cardiomyopathy. Adapted with permission from Ho. Data from Gersh et al.
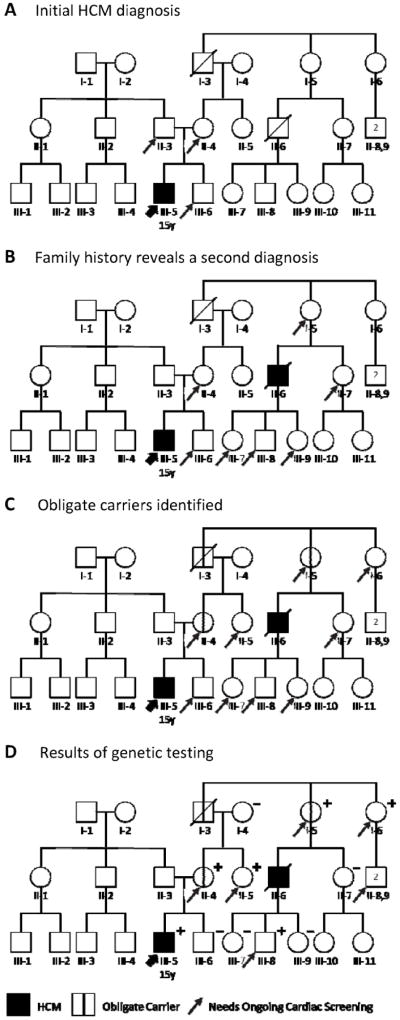
An evolving HCM family history, and careful pedigree assessment, shifts cardiology screening needs. A, Relatives needing screening based on initial diagnosis. Diagnosis of this 15-year-old patient (III-5, thick arrow) with HCM means his first-degree relatives (father II-3, mother II-4, and brother III-6; thin arrows) are each at 50% risk. B, Relatives needing screening based on initial plus a second diagnosis. When a second HCM diagnosis (II-6) is discovered in the patient’s maternal family history, this individual’s first-degree relatives (I-5, II-7, III-7, III-8, and III-9) also require cardiac screening. The patient’s father (II-3), not on the affected side of the family, is no longer considered at risk. C, Additional relatives need screening based on obligate carriers. Pedigree analysis identifies three obligate carriers (I-3, I-5, and II-4; marked with vertical line) connecting the individuals with HCM, including the patient’s mother. Each is at known risk for disease. Immediate family members of an obligate carrier are at 50% risk and also require screening (arrows added to I-6 and II-5). D, Genetic testing helps target screening to relatives definitively predisposed to HCM. In this family, several family members at 50% risk (II-7, III-6, III-7, and III-9) did not inherit the disease-causing variant; they and their descendants can be excused from further screening. By contrast, II-5 and I-6 test positive, newly revealing their children (II-8,9) to be at 50% risk. Circles indicate females; squares, males; slash, deceased; +, genetic variant present; –, genetic variant absent. HCM = hypertrophic cardiomyopathy. Adapted with permission from Ho.
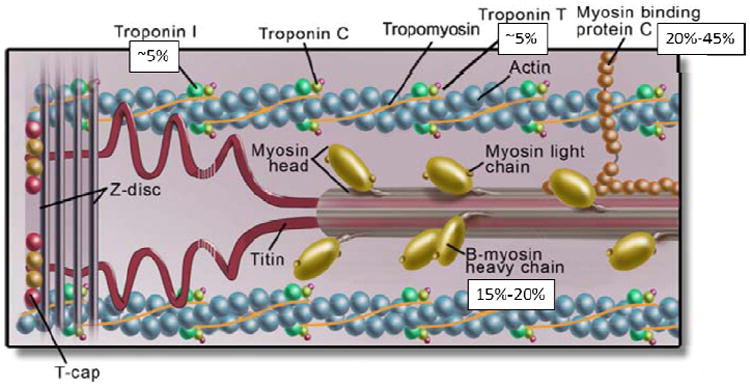
The cardiac sarcomere, highlighting protein products of genes involved in hypertrophic cardiomyopathy. Disease-causing variants in cardiac myosin-binding protein C (MYBPC3) and beta-myosin heavy chain (MYH7) are most common, accounting for 20-45% and 15-20% of the disease respectively. Cardiac troponin T type 2 (TNNT2) and troponin I type 3 (TNNI3) each account for ~5%. Variation in other sarcomere genes is less frequent. Data from Ackerman et al.
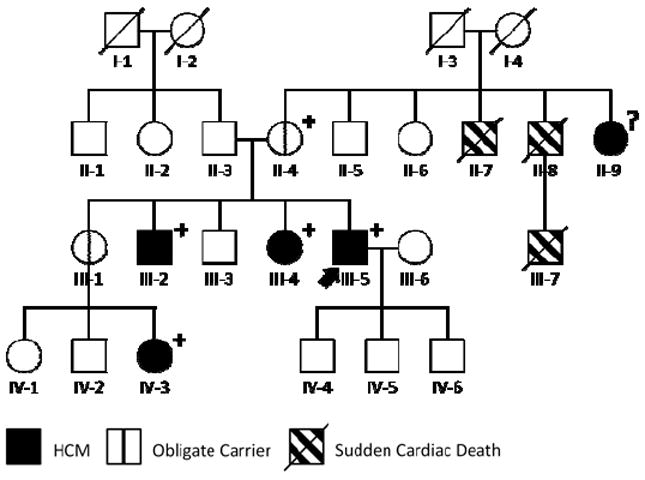
Robust segregation analysis can help to determine whether a specific genetic variant is responsible for disease. In this HCM family, genetic testing of our patient (arrow) revealed a variant of uncertain significance (VUS) in the MYH7 gene. The VUS was present in all affected family members (III-2, III-4, III-5, and IV-3) and obligate carriers (II-4) tested, increasing confidence in its pathogenicity. Circles indicate females; squares, males; slash, deceased; ?, genotype unknown; +, VUS present; −, VUS absent. HCM = hypertrophic cardiomyopathy.
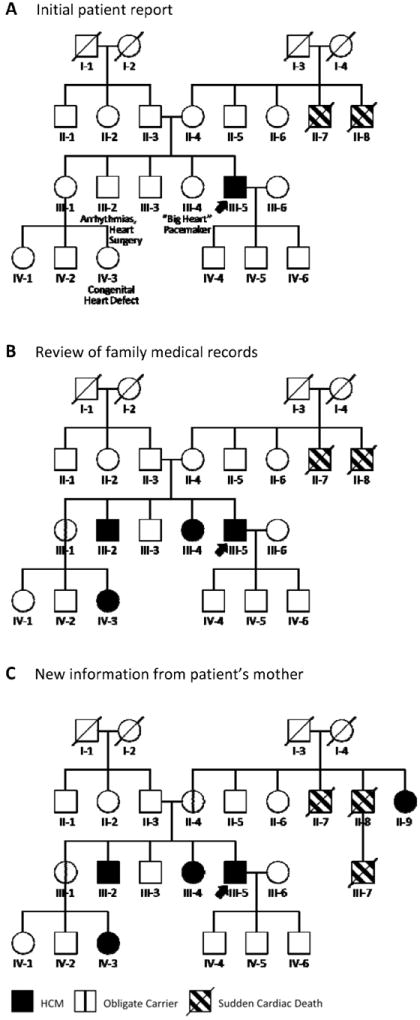
Constructing a family history is a dynamic process that unfolds over time. A, At diagnosis, this patient (arrow) had no known history of HCM but reported suspicious cardiac features in three family members (III-2, III-4, and IV-3). B, Review of family medical records dramatically altered the original history, showing those three family members to have HCM and the patient’s unaffected sister (III-1) to be an obligate carrier (vertical line). C, The patient’s mother then reported that her sister (II-9) carried a diagnosis of HCM. This definitively localized the disease to the maternal side of the family, revealing the patient’s mother (II-4) as another obligate carrier. Circles indicate females; squares, males; slash, deceased. HCM = hypertrophic cardiomyopathy.
References
-
- Watson JD, Crick FH. Molecular structure of nucleic acids; a structure for deoxyribose nucleic acid. Nature. 1953;171:737–738. - PubMed
-
- Hershberger RE, Lindenfeld J, Mestroni L, Seidman CE, Taylor MR, Towbin JA. Genetic evaluation of cardiomyopathy—a Heart Failure Society of America practice guideline. J Card Fail. 2009;15:83–97. - PubMed
-
- Maron BJ. Sudden death in young athletes. N Engl J Med. 2003;349:1064–1075. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
