

Effects of physical tracing on estimates of loss to follow-up, mortality and retention in low and middle income country antiretroviral therapy programs: a systematic review
- PMID: 23424643
- PMCID: PMC3570556
- DOI: 10.1371/journal.pone.0056047
Effects of physical tracing on estimates of loss to follow-up, mortality and retention in low and middle income country antiretroviral therapy programs: a systematic review
Abstract
Background: A large proportion of patients receiving antiretroviral therapy (ART) in low and middle income countries (LMICs) have unknown treatment outcomes and are classified as lost to follow-up (LTFU). Physical tracing of patients classified as LTFU is common; however, effects of tracing on outcomes remains unclear. The objective of this systematic review is to compare estimates of LTFU, mortality and retention in LMIC in cohorts of patients with and without physical tracing.
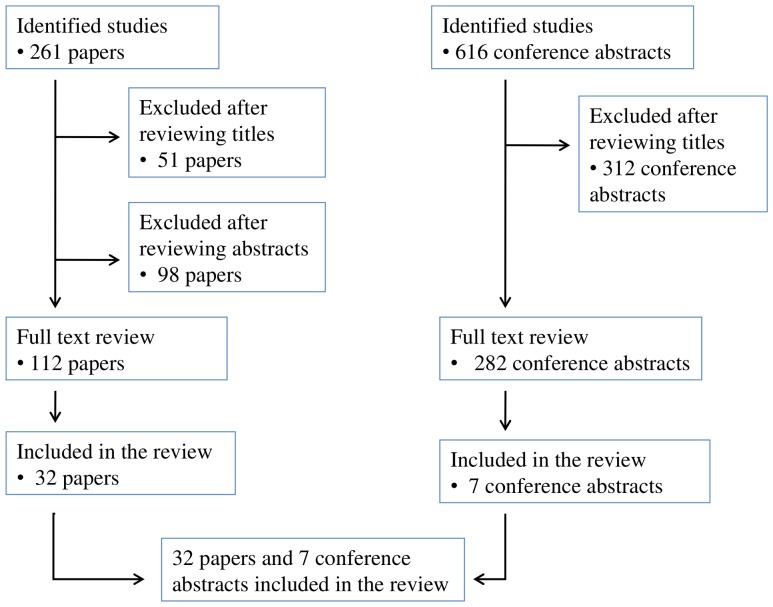
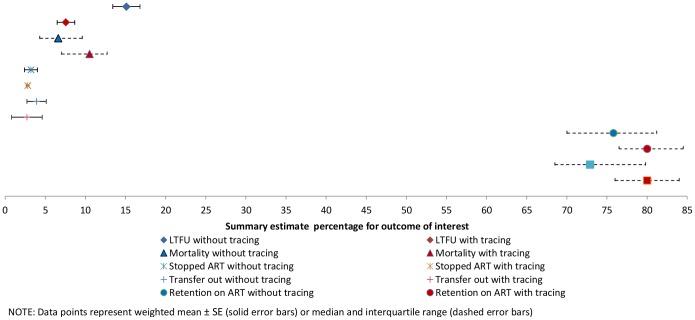
Methods and findings: We systematically identified studies in LMIC programmatic settings using MEDLINE (2003-2011) and HIV conference abstracts (2009-2011). Studies reporting the proportion LTFU 12-months after ART initiation were included. Tracing activities were determined from manuscripts or by contacting study authors. Studies were classified as "tracing studies" if physical tracing was available for the majority of patients. Summary estimates from the 2 groups of studies (tracing and non-tracing) for LTFU, mortality, stop of ART, transfers out, and retention on ART were determined. 261 papers and 616 abstracts were identified of which 39 studies comprising 54 separate cohorts (n = 187,666) met inclusion criteria. Of those, physical tracing was available for 46% of cohorts. Treatment programs with physical tracing activities had lower estimated LTFU (7.6% vs. 15.1%; p<.001), higher estimated mortality (10.5% vs. 6.6%; p = .006), higher retention on ART (80.0 vs. 75.8%; p = .04) and higher retention at the original site (80.0% vs. 72.9%; p = .02).
Conclusions: Knowledge of patient tracing is critical when interpreting program outcomes of LTFU, mortality and retention. The reduction of the proportion LTFU in tracing studies was only partially explained by re-classification of unknown outcomes. These data suggest that tracing may lead to increased re-engagement of patients in care, rather than just improved classification of unknown outcomes.
Conflict of interest statement
Figures
References
-
- WHO (2011) Towards universal access : scaling up priority HIV/AIDS interventions in the health sector : progress report 2011. Geneva: World Health Organization.
-
- Weidle PJ, Malamba S, Mwebaze R, Sozi C, Rukundo G, et al. (2002) Assessment of a pilot antiretroviral drug therapy programme in Uganda: patients' response, survival, and drug resistance. Lancet 360: 34–40. - PubMed
-
- Severe P, Leger P, Charles M, Noel F, Bonhomme G, et al. (2005) Antiretroviral therapy in a thousand patients with AIDS in Haiti. N Engl J Med 353: 2325–2334. - PubMed
-
- Coetzee D, Hildebrand K, Boulle A, Maartens G, Louis F, et al. (2004) Outcomes after two years of providing antiretroviral treatment in Khayelitsha, South Africa. AIDS 18: 887–895. - PubMed
-
- WHO (2010) HIV Drug Resistance Early Warning Indicators.World Health Organization indicators to monitor HIV drug resistance prevention at antiretroviral treatment sites. June 2010 Update. Geneva: World Health Organization.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
