

Cardiac output response to exercise in relation to metabolic demand in heart failure with preserved ejection fraction
- PMID: 23426022
- PMCID: PMC3857919
- DOI: 10.1093/eurjhf/hft026
Cardiac output response to exercise in relation to metabolic demand in heart failure with preserved ejection fraction
Abstract
Aims: Exercise intolerance is a hallmark of heart failure with preserved ejection fraction (HFpEF), yet its mechanisms remain unclear. The current study sought to determine whether increases in cardiac output (CO) during exercise are appropriately matched to metabolic demands in HFpEF.
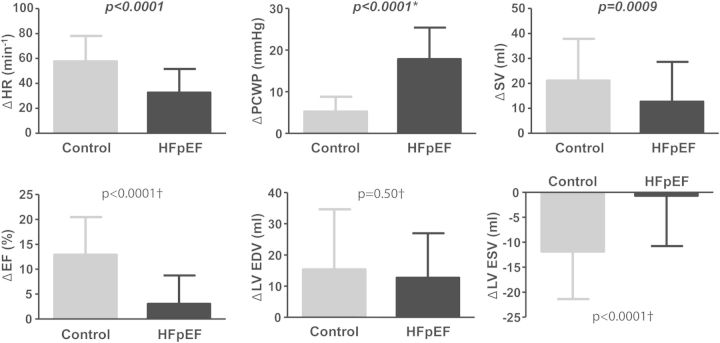
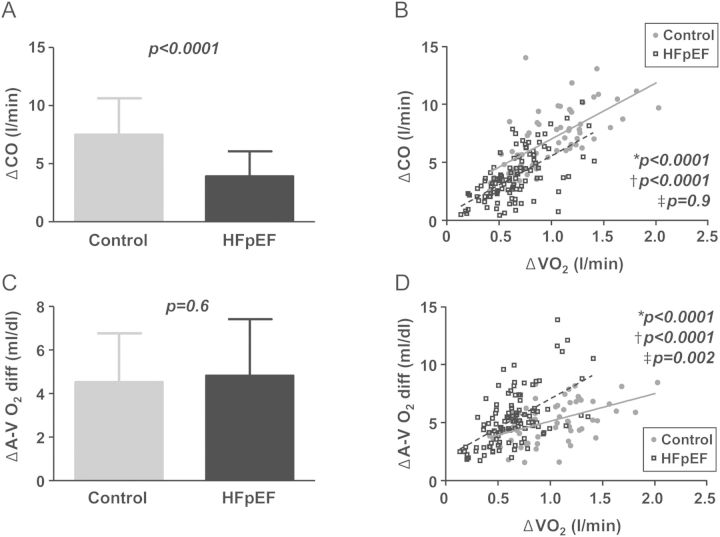
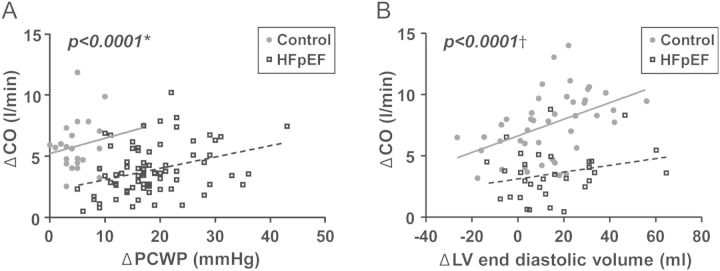
Methods and results: Patients with HFpEF (n = 109) and controls (n = 73) exercised to volitional fatigue with simultaneous invasive (n = 96) or non-invasive (n = 86) haemodynamic assessment and expired gas analysis to determine oxygen consumption (VO2) during upright or supine exercise. At rest, HFpEF patients had higher LV filling pressures but similar heart rate, stroke volume, EF, and CO. During supine and upright exercise, HFpEF patients displayed lower peak VO2 coupled with blunted increases in heart rate, stroke volume, EF, and CO compared with controls. LV filling pressures increased dramatically in HFpEF patients, with secondary elevation in pulmonary artery pressures. Reduced peak VO2 in HFpEF patients was predominantly attributable to CO limitation, as the slope of the increase in CO relative to VO2 was 20% lower in HFpEF patients (5.9 ± 2.5 vs. 7.4 ± 2.6 L blood/L O2, P = 0.0005). While absolute increases in arterial-venous O2 difference with exercise were similar in HFpEF patients and controls, augmentation in arterial-venous O2 difference relative to VO2 was greater in HFpEF patients (8.9 ± 3.4 vs. 5.5 ± 2.0 min/dL, P < 0.0001). These differences were observed in the total cohort and when upright and supine exercise modalities were examined individually.
Conclusion: While diastolic dysfunction promotes congestion and pulmonary hypertension with stress in HFpEF, reduction in exercise capacity is predominantly related to inadequate CO relative to metabolic needs.
Keywords: Cardiac output; Diastolic heart failure; Exercise; Heart rate; Oxygen consumption; Stroke volume.
Figures
References
-
- Denolin H, Kuhn H, Krayenbuehl HP, Loogen F, Reale A. The definition of heart failure. Eur Heart J. 1983;4:445–448. - PubMed
-
- Chomsky DB, Lang CC, Rayos GH, Shyr Y, Yeoh TK, Pierson RN, 3rd, Davis SF, Wilson JR. Hemodynamic exercise testing. A valuable tool in the selection of cardiac transplantation candidates. Circulation. 1996;94:3176–3183. - PubMed
-
- Sullivan MJ, Knight JD, Higginbotham MB, Cobb FR. Relation between central and peripheral hemodynamics during exercise in patients with chronic heart failure. Muscle blood flow is reduced with maintenance of arterial perfusion pressure. Circulation. 1989;80:769–781. - PubMed
-
- Lang CC, Agostoni P, Mancini DM. Prognostic significance and measurement of exercise-derived hemodynamic variables in patients with heart failure. J Card Fail. 2007;13:672–679. - PubMed
-
- Dexter L, Whittenberger JL, Haynes FW, Goodale WT, Gorlin R, Sawyer CG. Effect of exercise on circulatory dynamics of normal individuals. J Appl Physiol. 1951;3:439–453. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
