

Treating rural pediatric obesity through telemedicine: outcomes from a small randomized controlled trial
- PMID: 23428652
- PMCID: PMC3785218
- DOI: 10.1093/jpepsy/jst005
Treating rural pediatric obesity through telemedicine: outcomes from a small randomized controlled trial
Abstract
Objective: The objective of the current study was to examine the effectiveness of a multidisciplinary weekly family-based behavioral group delivered via telemedicine to rural areas, compared with a standard physician visit intervention.
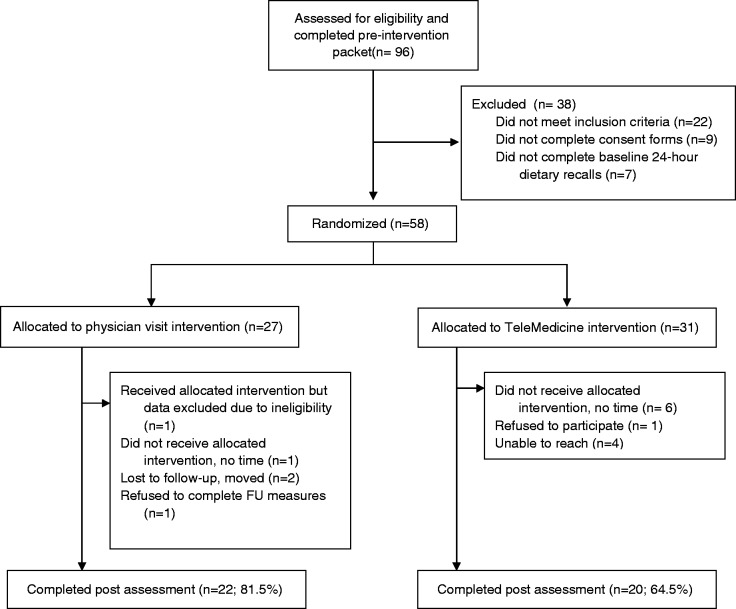
Methods: A randomized controlled trial was conducted with 58 rural children and their families comparing a family-based behavioral intervention delivered via telemedicine to a structured physician visit condition. Outcome measures included child body mass index z-score (BMIz), 24-hr dietary recalls, accelerometer data, Child Behavior Checklist, Behavioral Pediatrics Feeding Assessment Scale, and feasibility and fidelity.
Results: Child BMIz outcomes were not statistically different between the 2 groups (F = 0.023, p = .881). Improvements in BMIz, nutrition, and physical activity were seen for both groups.
Conclusions: Both telemedicine and structured physician visit may be feasible and acceptable methods of delivering pediatric obesity treatment to rural children.
Keywords: obesity; randomized controlled trial; weight management.
Figures
References
-
- Achenbach T M. Manual for the child behavior checklist/4–18 and 1991 profile. Burlington, VT: University of Vermont, Department of Psychiatry; 1991.
-
- Barlow S E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120(Suppl 4):S164–S192. Retrieved from http://pediatrics.aappublications.org/content/120/Supplement_4/S164.full.... - PubMed
-
- Centers for Disease Control and Prevention, National Center for Health Statistics. 2000 CDC growth charts: United States. Retrieved from http://www.cdc.gov/growthcharts.
-
- Crawford P B, Obarzanek E, Morrison J, Sabry Z I. Comparative advantage of 3-day food records over 24-hour recall and 5-day food frequency validated by observation of 9- and 10-year-old girls. Journal of the American Dietetic Asociation. 1994;94:626–630. doi:10.1016/0002-8223(94)90158-9. - PubMed
-
- Crist W, Dobbelsteyn C, Brousseau A M, Napier-Phillips A. Pediatric assessment scale for severe feeding problems: Validity and reliability of a new scale for tube-fed children. Nutrition in Clinical Practice. 2004;19:403–408. doi:10.1177/0115426504019004403. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
