

Rethinking Ormond's disease: "idiopathic" retroperitoneal fibrosis in the era of IgG4-related disease
- PMID: 23429355
- PMCID: PMC4553983
- DOI: 10.1097/MD.0b013e318289610f
Rethinking Ormond's disease: "idiopathic" retroperitoneal fibrosis in the era of IgG4-related disease
Abstract
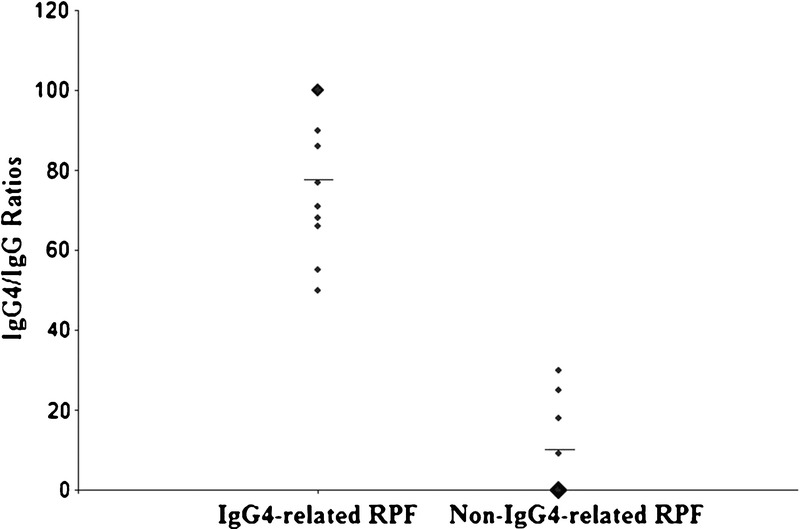
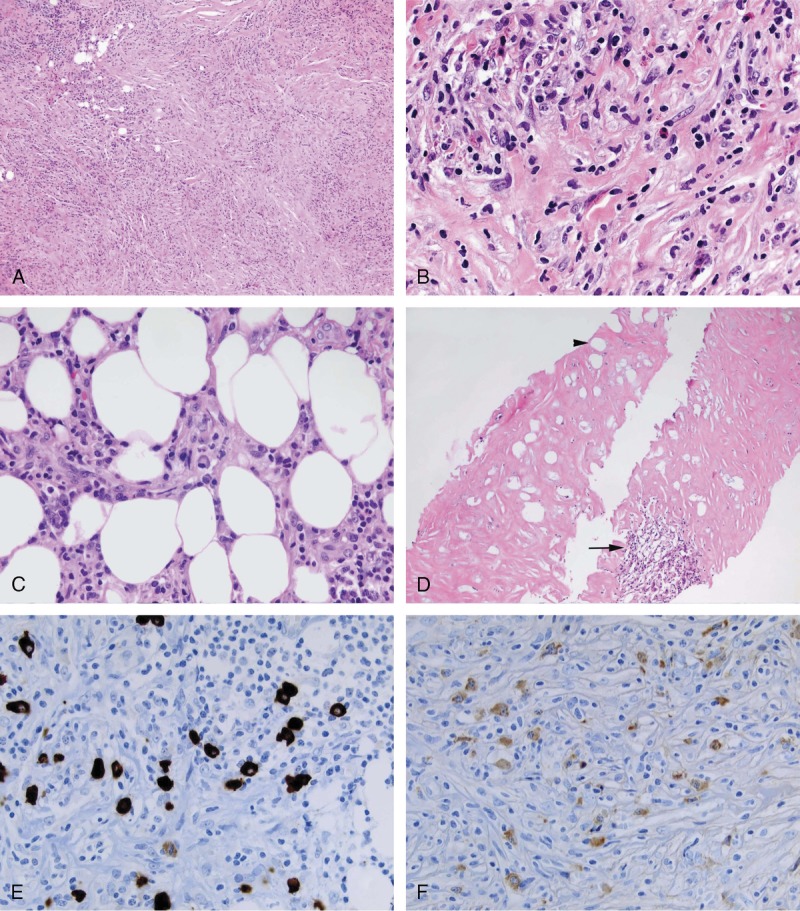
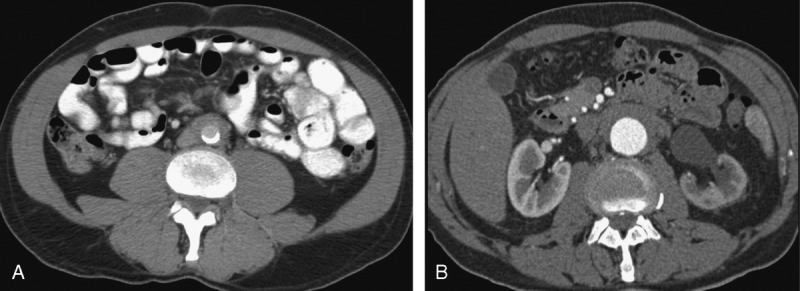
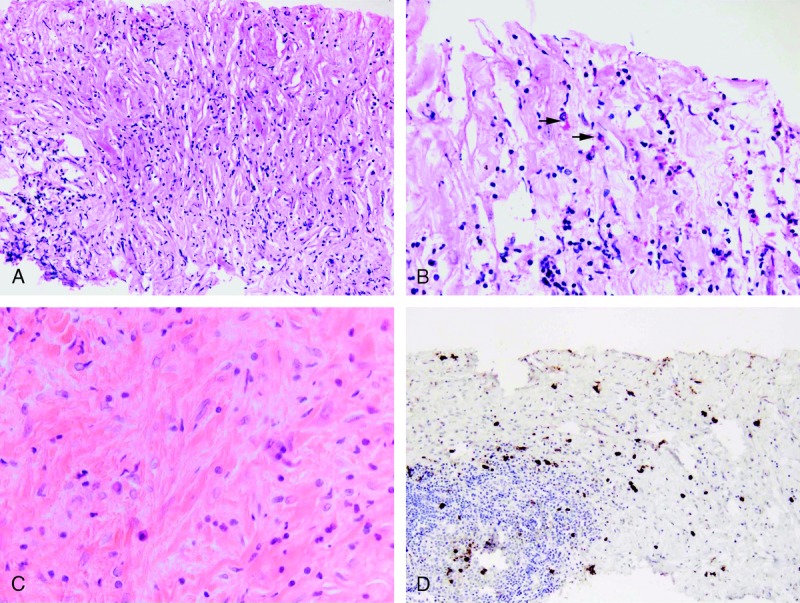
Idiopathic retroperitoneal fibrosis (RPF) is a periaortic sclerotic disease that encases adjacent retroperitoneal structures, particularly the ureters. A subset of idiopathic RPF cases can be associated with IgG4-related disease, but the frequency of this association is not clear. We selected 23 cases of idiopathic RPF and identified IgG4-related RPF cases based on the presence of IgG4+ plasma cells in the tissue, using an IgG4/IgG ratio cutoff of >40%. We then compared the IgG4-related RPF patients and the non-IgG4-related RPF patients in terms of both the presence of histopathologic features typical of IgG4-related disease and the simultaneous occurrence (or history) of other organ manifestations typical of IgG4-related disease. The IgG4-related RPF and non-IgG4-related RPF groups were also analyzed in terms of clinical, laboratory, and radiologic features and treatment review. We identified 13 cases of IgG4-related RPF (57% of the total cohort). The distinguishing features of IgG4-related RPF were histopathologic and extra-organ manifestations of IgG4-related disease. The IgG4-related RPF patients were statistically more likely than non-IgG4-related RPF patients to have retroperitoneal biopsies showing lymphoplasmacytic infiltrate (p = 0.006), storiform fibrosis (p = 0.006), or tissue eosinophilia (p = 0.0002). Demographics of the 2 groups, including a middle-aged, male predominance (mean age, 58 yr; 73% male), were similar. IgG4-related disease accounts for a substantial percentage of patients with "idiopathic" RPF. Histopathologic features such as storiform fibrosis, obliterative phlebitis, and tissue eosinophilia are critical to identifying this disease association. Extraretroperitoneal manifestations of IgG4-related disease are also often present among patients with IgG4-related RPF. Elevated IgG4/total IgG ratios in tissue biopsies are more useful than the number of IgG4+ plasma cells per high-power field in cases of RPF that are highly fibrotic.
Conflict of interest statement
The other authors have no funding or conflicts of interest to disclose.
Figures
References
-
- Carruthers MN, Stone JH, Khosroshahi A. The latest on IgG4-RD: a rapidly emerging disease. Curr Opin Rheumatol. 2012; 24: 60– 69. - PubMed
-
- Comings DE, Skubi KB, Van Eyes J, Motulsky AG. Familial multifocal fibrosclerosis. Findings suggesting that retroperitoneal fibrosis, mediastinal fibrosis, sclerosing cholangitis, Riedel’s thyroiditis, and pseudotumor of the orbit may be different manifestations of a single disease. Ann Intern Med. 1967; 66: 884– 892. - PubMed
-
- Corradi D, Maestri R, Palmisano A, Bosio S, Greco P, Manenti L, Ferretti S, Cobelli R, Moroni G, Dei Tos AP, Buzio C, Vaglio A. Idiopathic retroperitoneal fibrosis: clinicopathologic features and differential diagnosis. Kidney Int. 2007; 72: 742– 753. - PubMed
-
- Dahlgren M, Khosroshahi A, Nielsen GP, Deshpande V, Stone JH. Riedel’s thyroiditis and multifocal fibrosclerosis are part of the IgG4-related systemic disease spectrum. Arthritis Care Res (Hoboken). 2010; 62: 1312– 1318. - PubMed
-
- Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, Kloppel G, Heathcote JG, Khosroshahi A, Ferry JA, Aalberse RC, Bloch DB, Brugge WR, Bateman AC, Carruthers MN, Chari ST, Cheuk W, Cornell LD, Fernandez-Del Castillo C, Forcione DG, Hamilos DL, Kamisawa T, Kasashima S, Kawa S, Kawano M, Lauwers GY, Masaki Y, Nakanuma Y, Notohara K, Okazaki K, Ryu JK, Saeki T, Sahani DV, Smyrk TC, Stone JR, Takahira M, Webster GJ, Yamamoto M, Zamboni G, Umehara H, Stone JH. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25: 1181– 1192. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
