

Latent class analysis identifies distinct phenotypes of primary graft dysfunction after lung transplantation
- PMID: 23429890
- PMCID: PMC3734891
- DOI: 10.1378/chest.12-1480
Latent class analysis identifies distinct phenotypes of primary graft dysfunction after lung transplantation
Abstract
Background: There is significant heterogeneity within the primary graft dysfunction (PGD) syndrome. We aimed to identify distinct grade 3 PGD phenotypes based on severity of lung dysfunction and patterns of resolution.
Methods: Subjects from the Lung Transplant Outcomes Group (LTOG) cohort study with grade 3 PGD within 72 h after transplantation were included. Latent class analysis (LCA) was used to statistically identify classes based on changes in PGD International Society for Heart & Lung Transplantation grade over time. Construct validity of the classes was assessed by testing for divergence of recipient, donor, and operative characteristics between classes. Predictive validity was assessed using time to death.
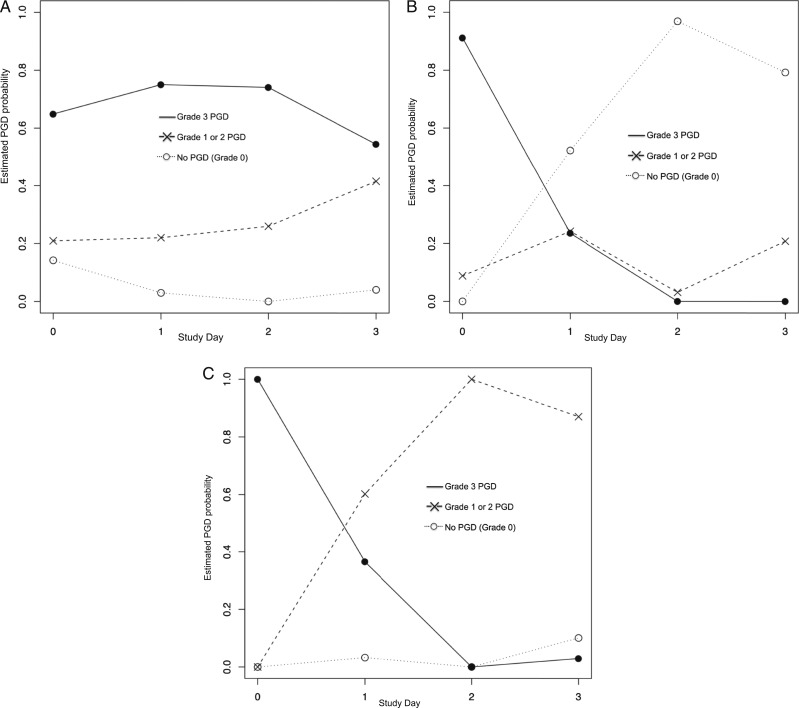
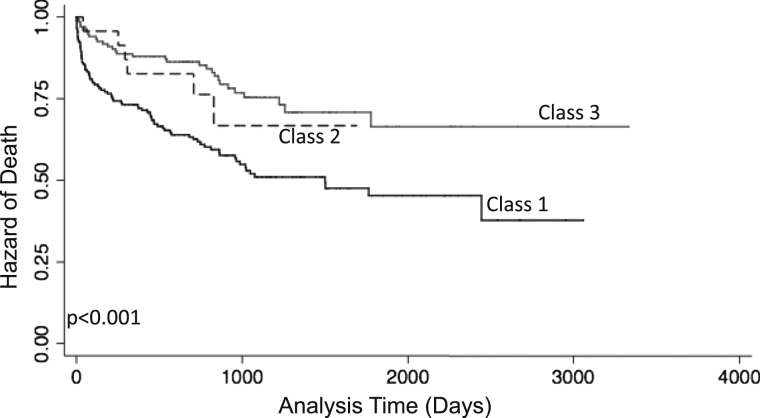
Results: Of 1,255 subjects, 361 had grade 3 PGD within the first 72 h after transplantation. LCA identified three distinct phenotypes: (1) severe persistent dysfunction (class 1), (2) complete resolution of dysfunction within 72 h (class 2), and (3) attenuation, without complete resolution within 72 h (class 3). Increased use of cardiopulmonary bypass, greater RBC transfusion, and higher mean pulmonary artery pressure were associated with persistent PGD (class 1). Subjects in class 1 also had the greatest risk of death (hazard ratio, 2.39; 95% CI, 1.57-3.63; P < .001).
Conclusions: There are distinct phenotypes of resolution of dysfunction within the severe PGD syndrome. Subjects with early resolution may represent a different mechanism of lung pathology, such as resolving pulmonary edema, whereas those with persistent PGD may represent a more severe phenotype. Future studies aimed at PGD mechanism or treatment may focus on phenotypes based on resolution of graft dysfunction.
Figures
Comment in
-
Distinct phenotypes of primary graft dysfunction after lung transplantation.Chest. 2014 Jan;145(1):192-193. doi: 10.1378/chest.13-1957. Chest. 2014. PMID: 24394843 No abstract available.
-
Response.Chest. 2014 Jan;145(1):193. doi: 10.1378/chest.13-2226. Chest. 2014. PMID: 24394844 Free PMC article. No abstract available.
References
-
- Christie JD, Kotloff RM, Pochettino A, et al. Clinical risk factors for primary graft failure following lung transplantation. Chest. 2003;124(4):1232-1241 - PubMed
-
- Christie JD, Carby M, Bag R, Corris P, Hertz M, Weill D; ISHLT Working Group on Primary Lung Graft Dysfunction Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part II: definition. A consensus statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2005;24(10):1454-1459 - PubMed
-
- Christie JD, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: Twenty-eighth Adult Lung and Heart-Lung Transplant Report—2011. J Heart Lung Transplant. 2011;30(10):1104-1122 - PubMed
-
- Dahlberg PS, Prekker ME, Herrington CS, Hertz MI, Park SJ. Medium-term results of extracorporeal membrane oxygenation for severe acute lung injury after lung transplantation. J Heart Lung Transplant. 2004;23(8):979-984 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
