

Contributors to diffusion impairment in HIV-infected persons
- PMID: 23429919
- PMCID: PMC4023348
- DOI: 10.1183/09031936.00157712
Contributors to diffusion impairment in HIV-infected persons
Abstract
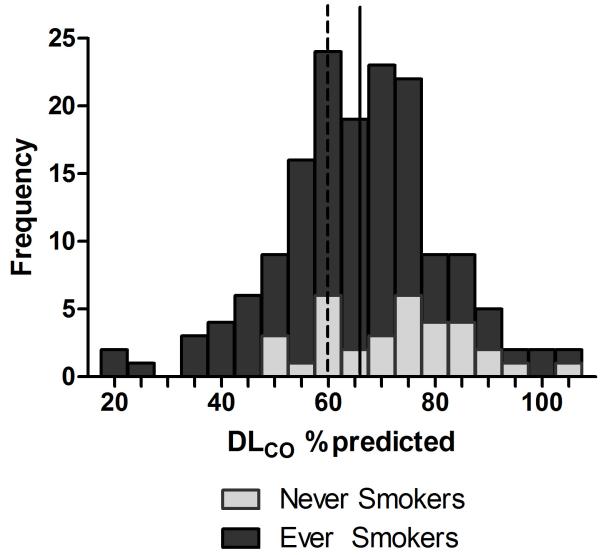
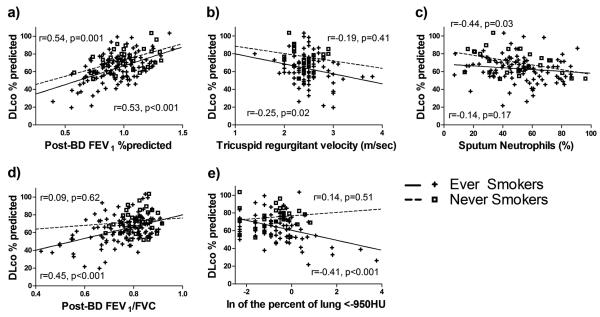
Abnormal diffusing capacity is common in HIV-infected individuals, including never smokers. Aetiologies for diffusing capacity impairment in HIV are not understood, particularly in those without a history of cigarette smoking. Our study was a cross-sectional analysis of 158 HIV-infected individuals without acute respiratory symptoms or infection with the aim to determine associations between a diffusing capacity of the lung for carbon monoxide (D(LCO)) % predicted and participant demographics, pulmonary spirometric measures (forced expiratory volume in 1 s (FEV1) and FEV1/forced vital capacity), radiographic emphysema (fraction of lung voxels < -950 Hounsfield units), pulmonary vascular/cardiovascular disease (echocardiographic tricuspid regurgitant jet velocity, N-terminal pro-brain natriuretic peptide) and airway inflammation (induced sputum cell counts), stratified by history of smoking. The mean D(LCO) was 65.9% predicted, and 55 (34.8%) participants had a significantly reduced D(LCO) (<60% predicted). Lower D(LCO) % predicted in ever-smokers was associated with lower post-bronchodilator FEV1 % predicted (p<0.001) and greater radiographic emphysema (p=0.001). In never-smokers, mean±SD D(LCO) was 72.7±13.4% predicted, and D(LCO) correlated with post-bronchodilator FEV1 (p=0.02), sputum neutrophils (p=0.03) and sputum lymphocytes (p=0.009), but not radiographic emphysema. Airway obstruction, emphysema and inflammation influence D(LCO) in HIV. Never-smokers may have a unique phenotype of diffusing capacity impairment. The interaction of multiple factors may account for the pervasive nature of diffusing capacity impairment in HIV infection.
Figures
References
-
- Louie JK, Hsu LC, Osmond DH, Katz MH, Schwarcz SK. Trends in causes of death among persons with Acquired Immunodeficiency Syndrome in the era of highly active antiretroviral therapy, San Francisco, 1994-1998. J Infect Dis. 2002;186(7):1023–7. - PubMed
-
- Diaz PT, King MA, Pacht ER, Wewers MD, Gadek JE, Neal D, Nagaraja HN, Drake J, Clanton TL. The pathophysiology of pulmonary diffusion impairment in human immunodeficiency virus infection. Am J Respir Crit Care Med. 1999;160(1):272–7. - PubMed
-
- Mitchell DM, Fleming J, Pinching AJ, Harris JR, Moss FM, Veale D, Shaw RJ. Pulmonary function in human immunodeficiency virus infection. A prospective 18-month study of serial lung function in 474 patients. Am Rev Respir Dis. 1992;146(3):745–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical