

Diagnosis and management of insulinoma
- PMID: 23430217
- PMCID: PMC3574879
- DOI: 10.3748/wjg.v19.i6.829
Diagnosis and management of insulinoma
Abstract
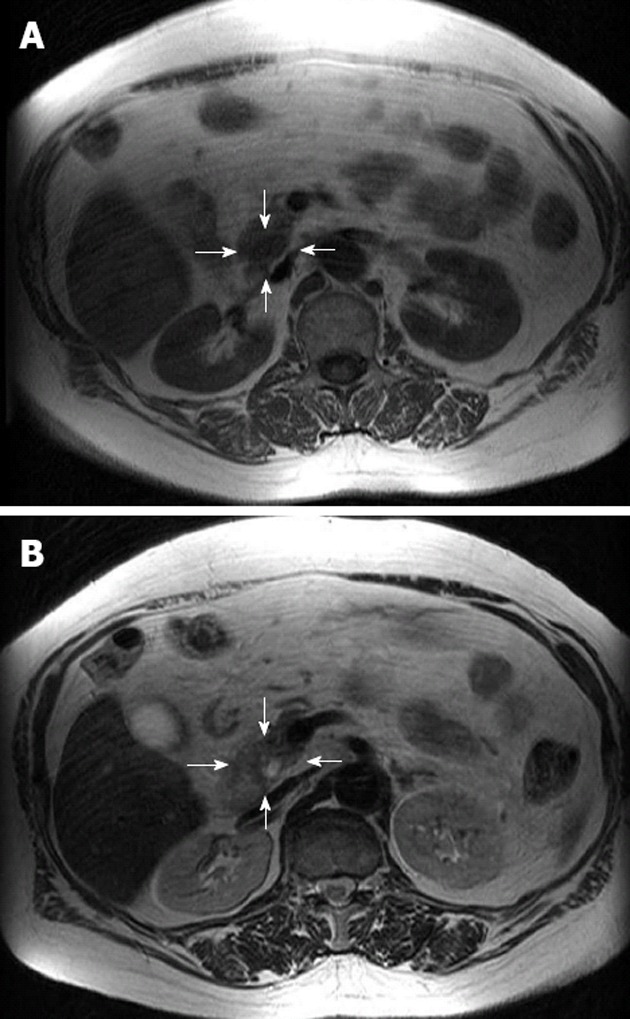
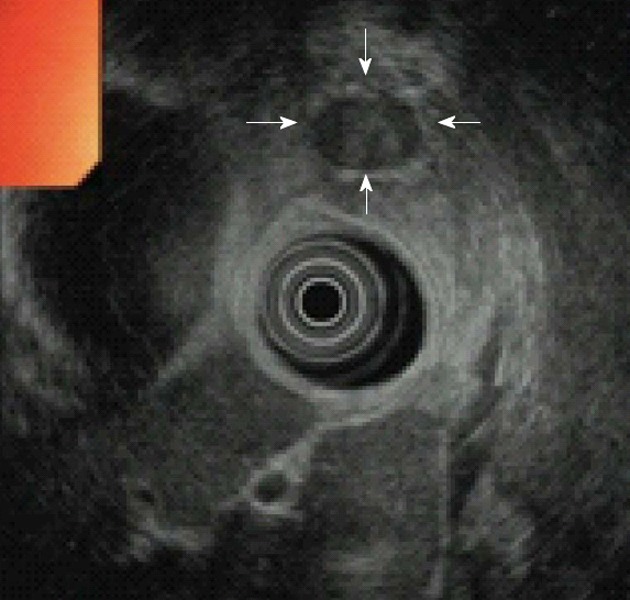
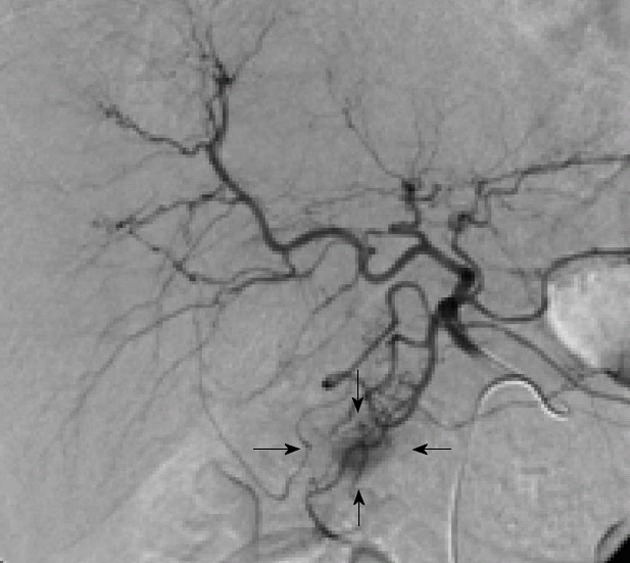
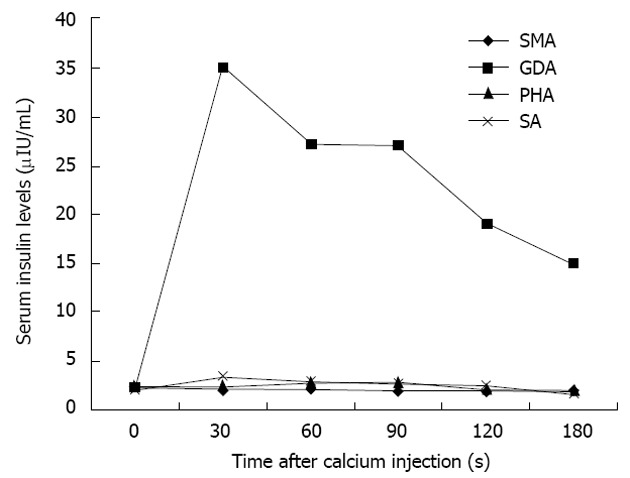
Insulinomas, the most common cause of hypoglycemia related to endogenous hyperinsulinism, occur in 1-4 people per million of the general population. Common autonomic symptoms of insulinoma include diaphroresis, tremor, and palpitations, whereas neuroglycopenenic symptoms include confusion, behavioural changes, personality changes, visual disturbances, seizure, and coma. Diagnosis of suspected cases is based on standard endocrine tests, especially the prolonged fasting test. Non-invasive imaging procedures, such as computed tomography and magnetic resonance imaging, are used when a diagnosis of insulinoma has been made to localize the source of pathological insulin secretion. Invasive modalities, such as endoscopic ultrasonography and arterial stimulation venous sampling, are highly accurate in the preoperative localization of insulinomas and have frequently been shown to be superior to non-invasive localization techniques. The range of techniques available for the localization of insulinomas means that blind resection can be avoided. Intraoperative manual palpation of the pancreas by an experienced surgeon and intraoperative ultrasonography are both sensitive methods with which to finalize the location of insulinomas. A high proportion of patients with insulinomas can be cured with surgery. In patients with malignant insulinomas, an aggressive medical approach, including extended pancreatic resection, liver resection, liver transplantation, chemoembolization, or radiofrequency ablation, is recommended to improve both survival and quality of life. In patients with unresectable or uncontrollable insulinomas, such as malignant insulinoma of the pancreas, several techniques should be considered, including administration of ocreotide and/or continuous glucose monitoring, to prevent hypoglycemic episodes and to improve quality of life.
Keywords: Continuous blood glucose monitoring; Diagnosis; Insulinoma; Management; Neuroendocrine pancreatic tumor; Pancreas.
Figures


References
-
- Moldow RE, Connelly RR. Epidemiology of pancreatic cancer in Connecticut. Gastroenterology. 1968;55:677–686. - PubMed
-
- Service FJ, McMahon MM, O’Brien PC, Ballard DJ. Functioning insulinoma--incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991;66:711–719. - PubMed
-
- Kimura W, Kuroda A, Morioka Y. Clinical pathology of endocrine tumors of the pancreas. Analysis of autopsy cases. Dig Dis Sci. 1991;36:933–942. - PubMed
-
- Lam KY, Lo CY. Pancreatic endocrine tumour: a 22-year clinico-pathological experience with morphological, immunohistochemical observation and a review of the literature. Eur J Surg Oncol. 1997;23:36–42. - PubMed
-
- Eriksson B, Oberg K. Neuroendocrine tumours of the pancreas. Br J Surg. 2000;87:129–131. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
