

Role of contrast-enhanced ultrasound in follow-up assessment after ablation for hepatocellular carcinoma
- PMID: 23430451
- PMCID: PMC3574882
- DOI: 10.3748/wjg.v19.i6.855
Role of contrast-enhanced ultrasound in follow-up assessment after ablation for hepatocellular carcinoma
Abstract
Aim: To assess the usefulness of contrast-enhanced ultrasound (CEUS) during follow-up after percutaneous ablation therapy for hepatocellular carcinoma (HCC).
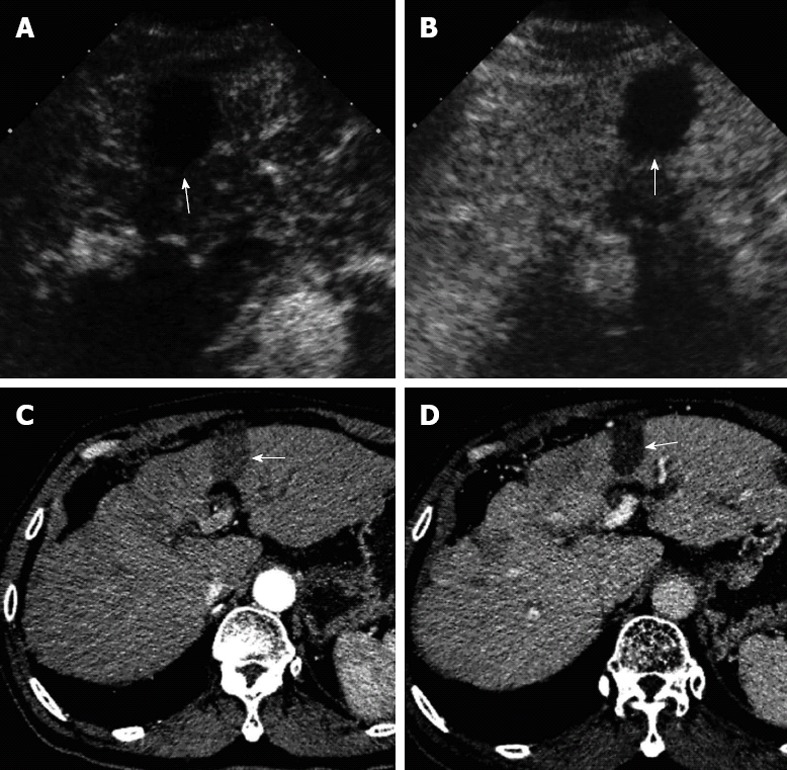
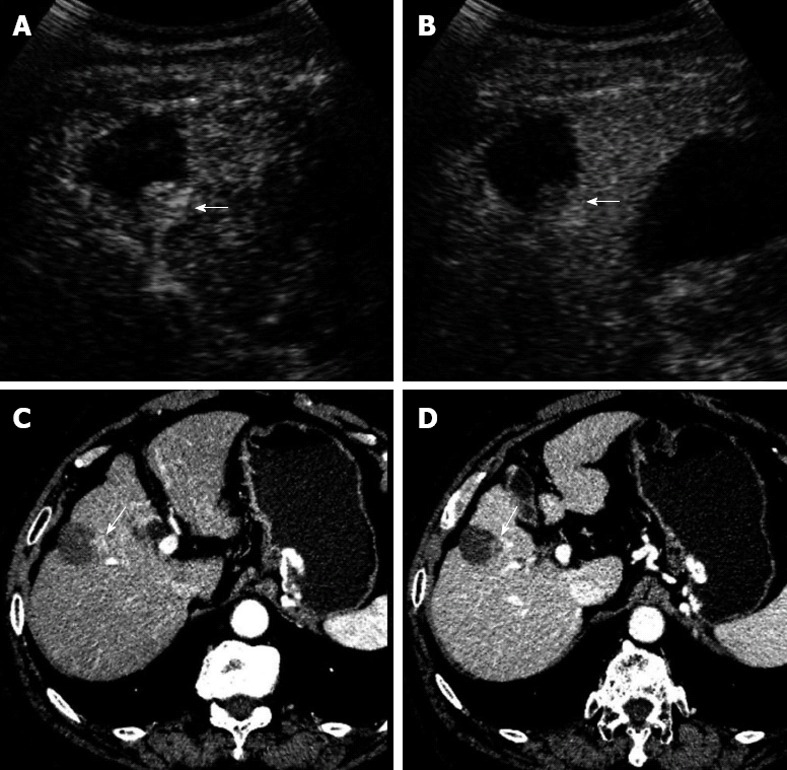
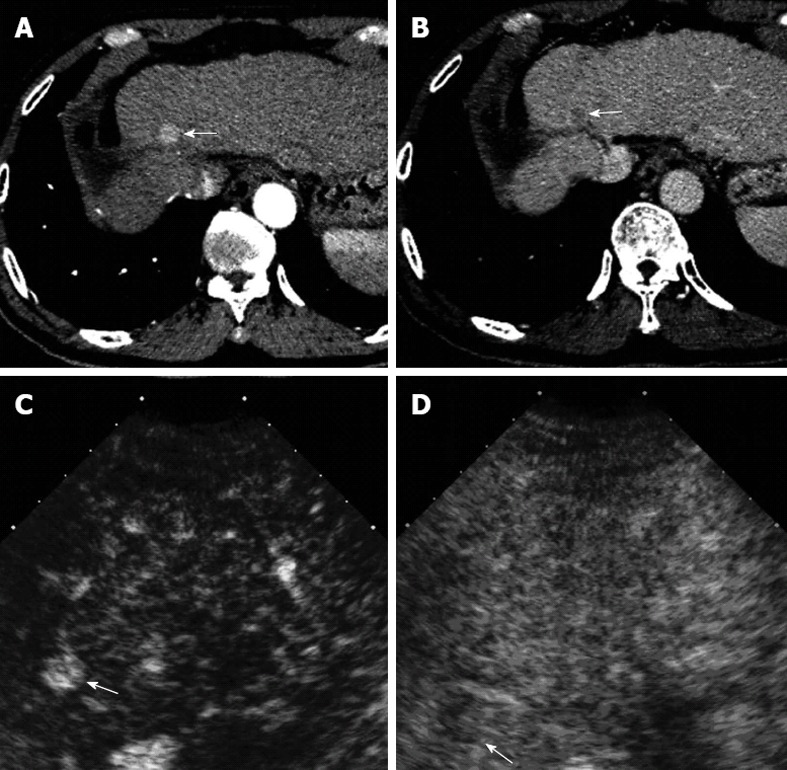
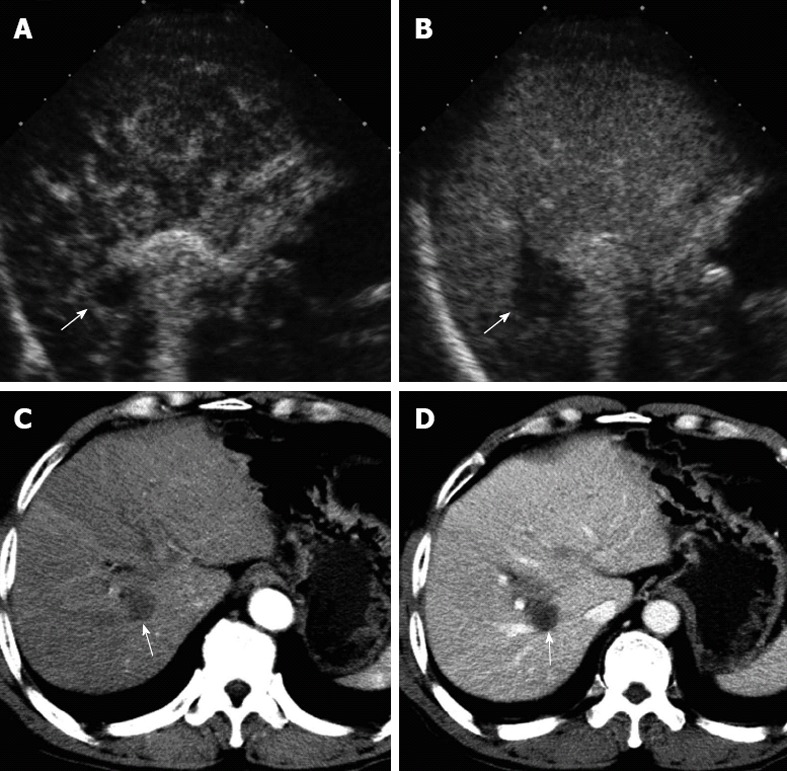
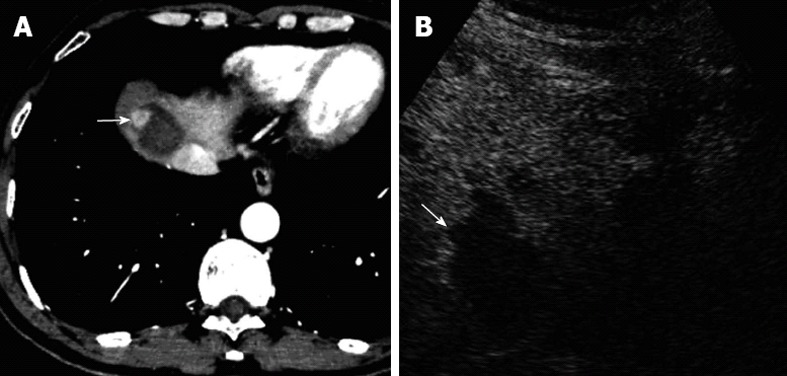
Methods: A total of 141 patients with HCCs who received percutaneous ablation therapy were assessed by paired follow-up CEUS and contrast-enhanced computed tomography (CECT). The follow-up scheme was designed prospectively and the intervals between CEUS and CECT examinations were less than 14 d. Both images of follow-up CEUS and CECT were reviewed by radiologists. The ablated lesions were evaluated and classified as local tumor progression (LTP) and LTP-free. LTP was defined as regrowth of tumor inside or adjacent to the successfully treated nodule. The detected new intrahepatic recurrences were also evaluated and defined as presence of intrahepatic new foci. On CEUS and CECT, LTP and new intrahepatic recurrence both were displayed as typical enhancement pattern of HCC (i.e., hyper-enhancing during the arterial phase and washout in the late phase). With CECT as the reference standard, the ability of CEUS in detecting LTP or new intrahepatic recurrence during follow-up was evaluated.
Results: During a follow-up period of 1-31 mo (median, 4 mo), 169 paired CEUS and CECT examinations were carried out for the 141 patients. For a total of 221 ablated lesions, 266 comparisons between CEUS and CECT findings were performed. Thirty-three LTPs were detected on CEUS whereas 40 LTPs were detected on CECT, there was significant difference (P < 0.001). In comparison with CECT, the numbers of false positive and false negative LTPs detected on CEUS were 6 and 13, respectively; the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and overall accuracy of CEUS in detecting LTPs were 67.5%, 97.4%, 81.8%, 94.4% and 92.3%, respectively. Meanwhile, 131 new intrahepatic recurrent foci were detected on CEUS whereas 183 were detected on CECT, there was also significant difference (P < 0.05). In comparison with CECT, the numbers of false positive and false negative intrahepatic recurrences detected on CEUS were 13 and 65, respectively; the sensitivity, specificity, PPV, NPV and overall accuracy of CEUS in detecting new intrahepatic recurrent foci were 77.7%, 92.0%, 92.4%, 76.7% and 84.0%, respectively.
Conclusion: The sensitivity of CEUS in detecting LTP and new intrahepatic recurrence after percutaneous ablation therapy is relatively low in comparison with CECT.
Keywords: Contrast-enhanced computed tomography; Contrast-enhanced ultrasound; Hepatocellular carcinoma; Microwave ablation; Radiofrequency ablation.
Figures
Comment in
-
Hepatocellular carcinoma after ablation: the imaging follow-up scheme.World J Gastroenterol. 2013 Feb 14;19(6):797-801. doi: 10.3748/wjg.v19.i6.797. World J Gastroenterol. 2013. PMID: 23429970 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Kim SK, Lim HK, Kim YH, Lee WJ, Lee SJ, Kim SH, Lim JH, Kim SA. Hepatocellular carcinoma treated with radio-frequency ablation: spectrum of imaging findings. Radiographics. 2003;23:107–121. - PubMed
-
- Llovet JM, Bruix J. Novel advancements in the management of hepatocellular carcinoma in 2008. J Hepatol. 2008;48 Suppl 1:S20–S37. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
