

Nutritional Changes and Micronutrient Supply in Patients with Phenylketonuria Under Therapy with Tetrahydrobiopterin (BH(4))
- PMID: 23430545
- PMCID: PMC3565664
- DOI: 10.1007/8904_2012_176
Nutritional Changes and Micronutrient Supply in Patients with Phenylketonuria Under Therapy with Tetrahydrobiopterin (BH(4))
Abstract
Background: Since 2008 patients with BH(4)-sensitive phenylketonuria can be treated with sapropterin dihydrochloride (Kuvan®) in addition to the classic phenylalanine (Phe) restricted diet. The aim of this study was to evaluate the nutritional changes and micronutrient supply in patients with phenylketonuria (PKU) under therapy with tetrahydrobiopterin (BH(4)).
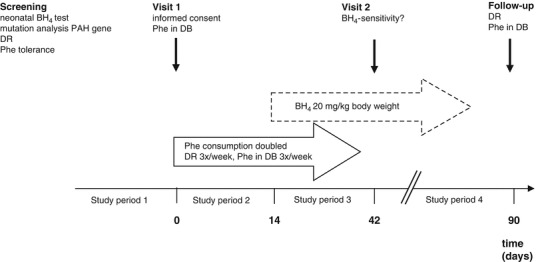
Subjects and methods: 19 children with PKU (4-18 years) and potential BH(4)-sensitivity were included, 14 completed the study protocol. Dried blood Phe concentrations as well as detailed dietary records were obtained throughout the study at preassigned study days.
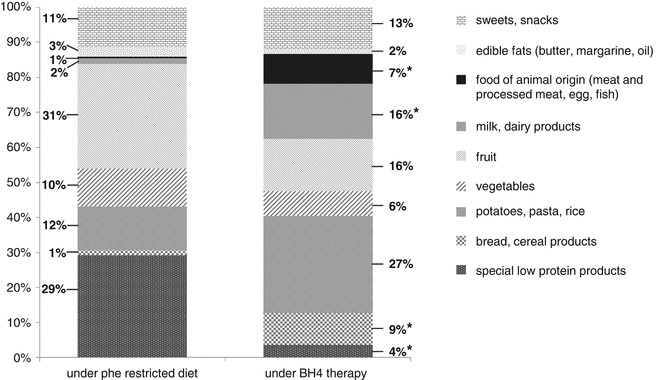
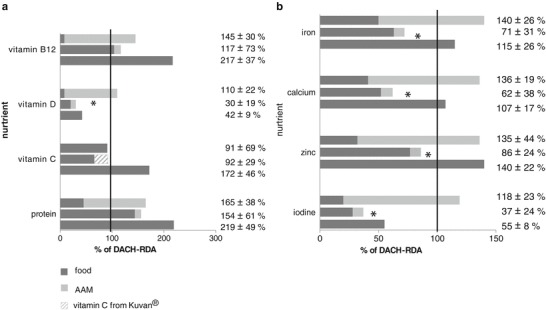
Results: Eight patients could increase their Phe tolerance from 629 ± 476 mg to 2131 ± 1084 mg (P = 0.006) under BH(4) while maintaining good metabolic control (Phe concentration in dried blood 283 ± 145 μM vs. 304 ± 136 μM, P = 1.0), therefore proving to be BH(4)-sensitive. They decreased their consumption of special low protein products and fruit while increasing their consumption of high protein foods such as processed meat, milk and dairy products. Intake of vitamin D (P = 0.016), iron (P = 0.002), calcium (P = 0.017), iodine (P = 0.005) and zinc (P = 0.046) significantly declined during BH(4) treatment while no differences in energy and macronutrient supply occurred.
Conclusion: BH(4)-sensitive patients showed good metabolic control under markedly increased Phe consumption. However, the insufficient supply of some micronutrients needs consideration. Long-term multicenter settings with higher sample sizes are necessary to investigate the changes of nutrient intake under BH(4) therapy to further evaluate potential risks of malnutrition. Supplementation may become necessary.
Figures
References
-
- Bélanger-Quintana A, García MJ, Castro M, Desviat LR, Pérez B, Mejía B, et al. Spanish BH4-responsive phenylalanine hydroxylase-deficient patients: evolution of seven patients on long-term treatment with tetrahydrobiopterin. Mol Genet Metab. 2005;86(Suppl 1):S61–S66. doi: 10.1016/j.ymgme.2005.07.024. - DOI - PubMed
LinkOut - more resources
Full Text Sources
