

Regression of albuminuria and hypertension and arrest of severe renal injury by a losartan-hydrochlorothiazide association in a model of very advanced nephropathy
- PMID: 23431367
- PMCID: PMC3576388
- DOI: 10.1371/journal.pone.0056215
Regression of albuminuria and hypertension and arrest of severe renal injury by a losartan-hydrochlorothiazide association in a model of very advanced nephropathy
Abstract
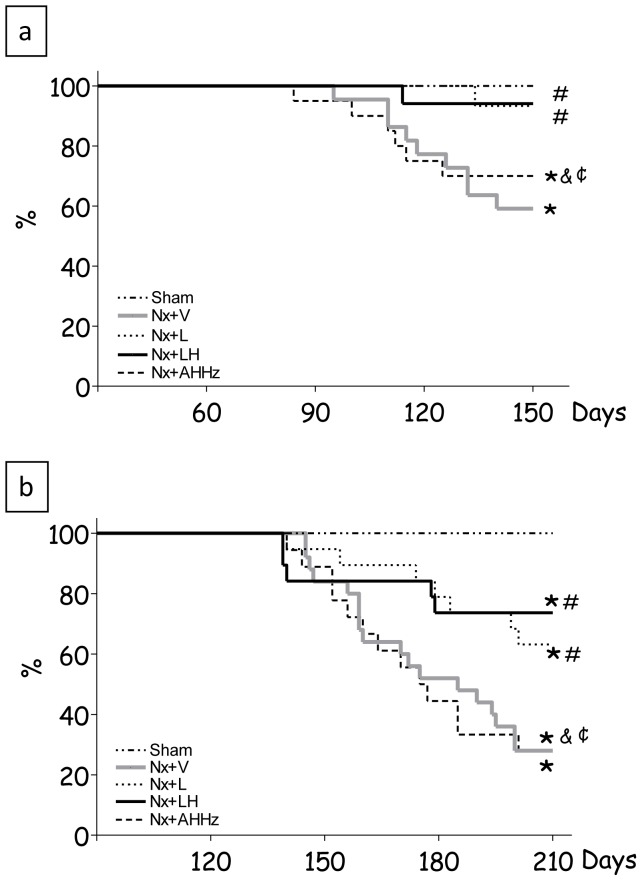
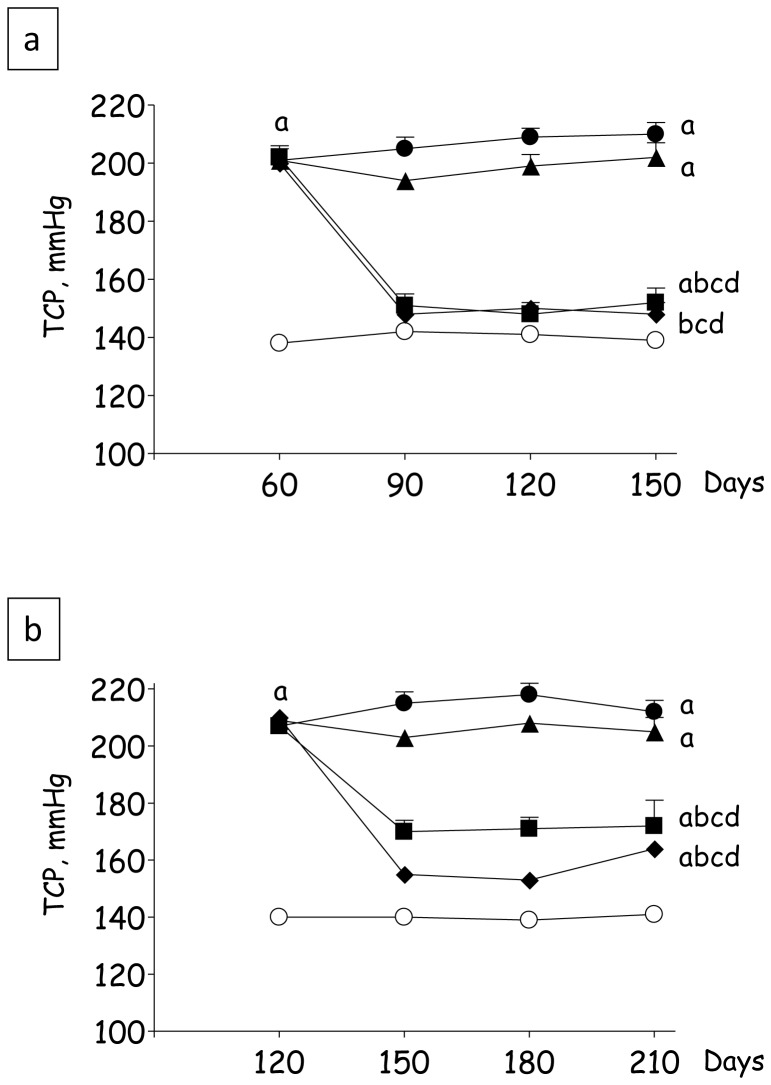
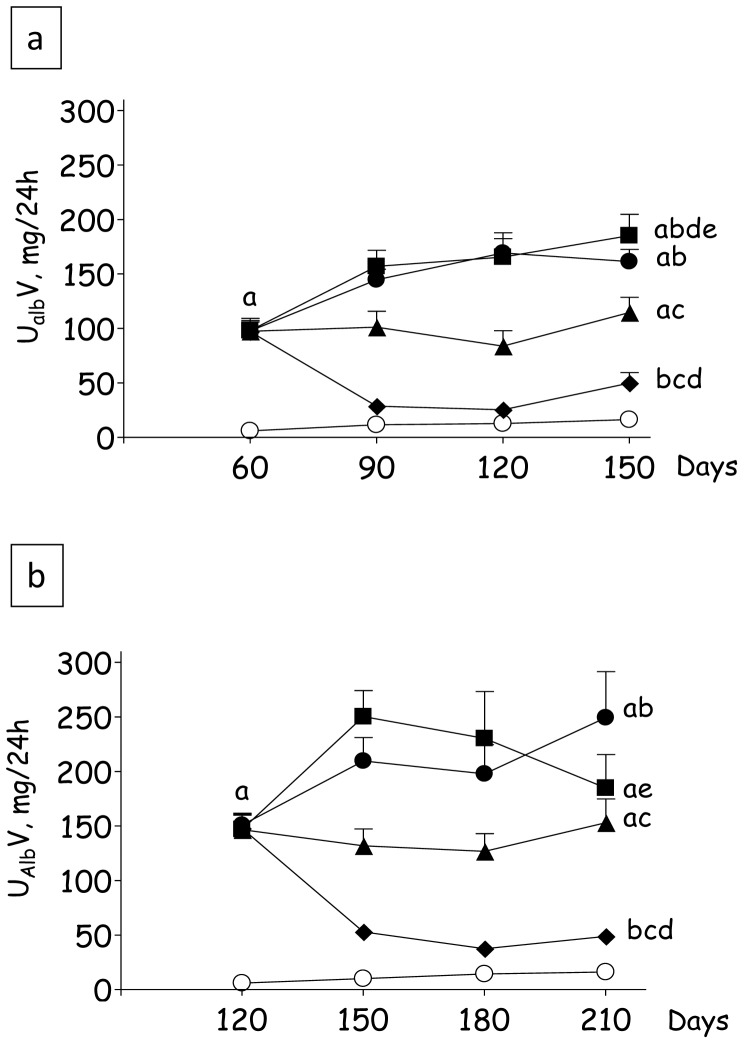
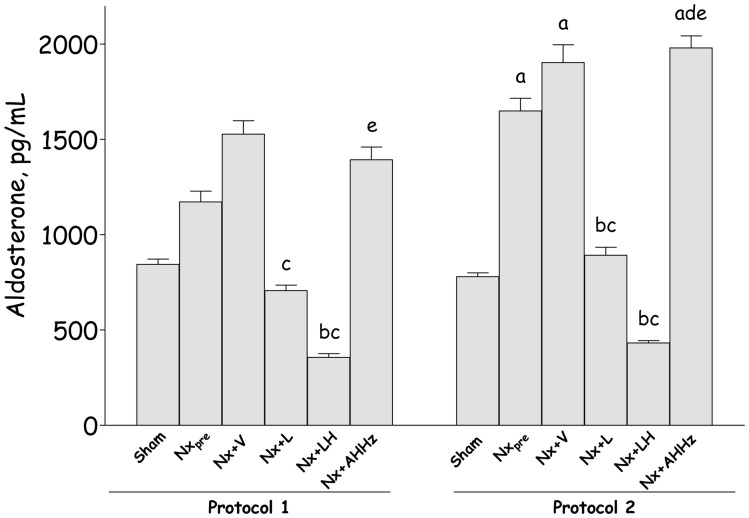
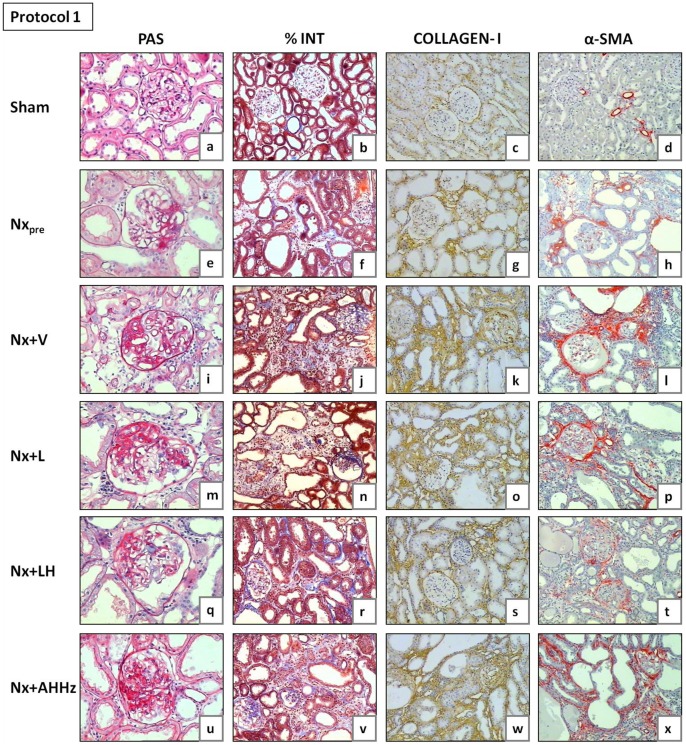
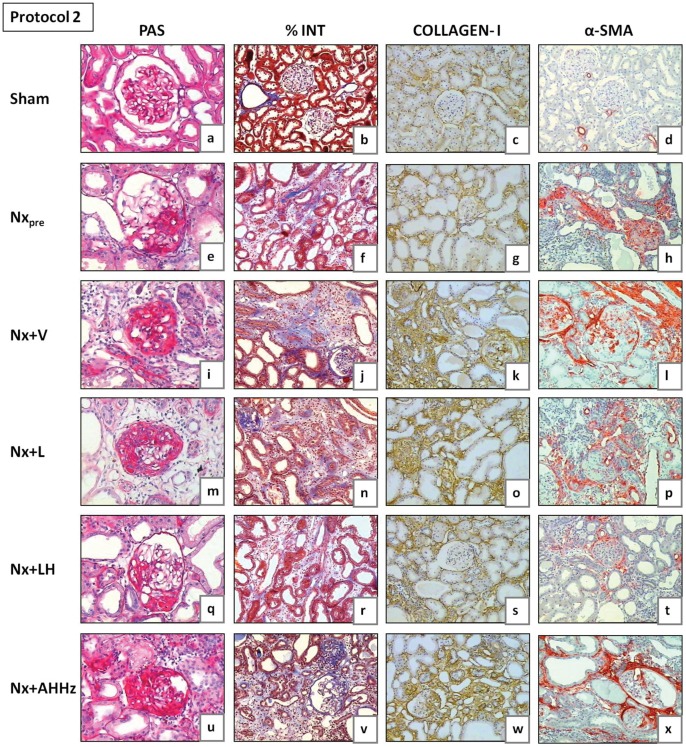
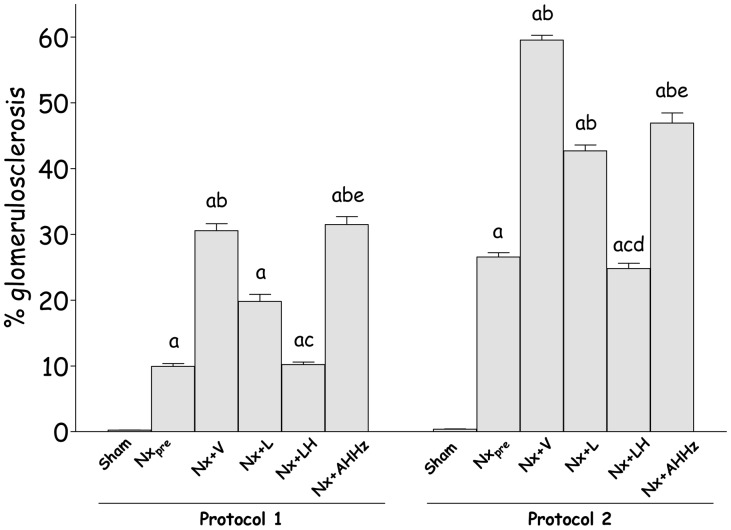
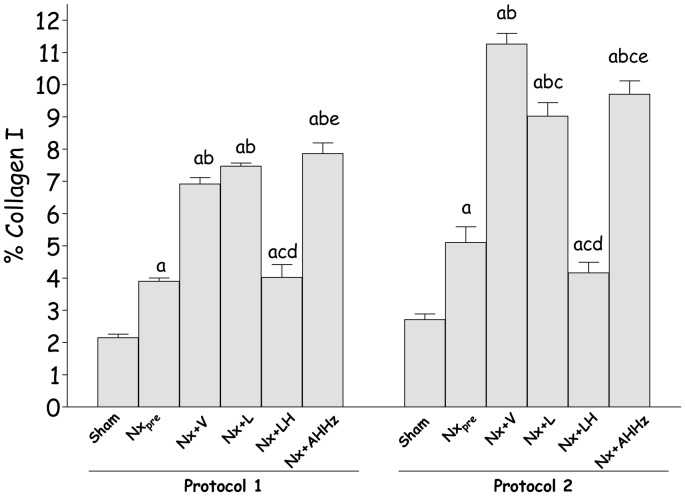
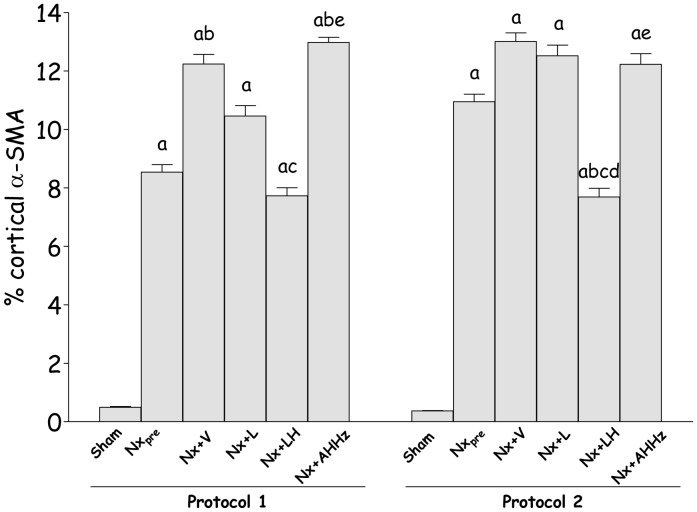
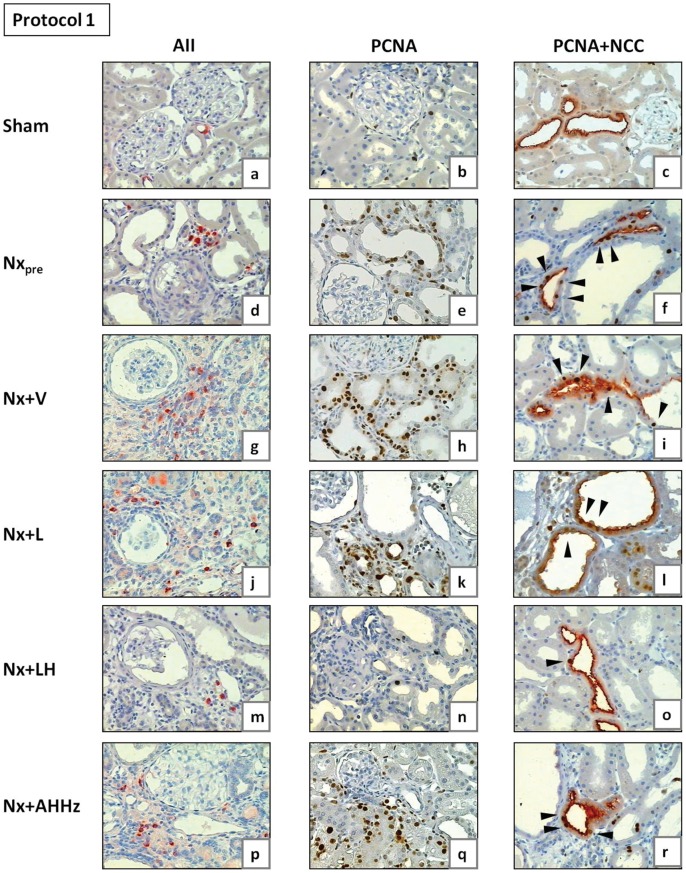
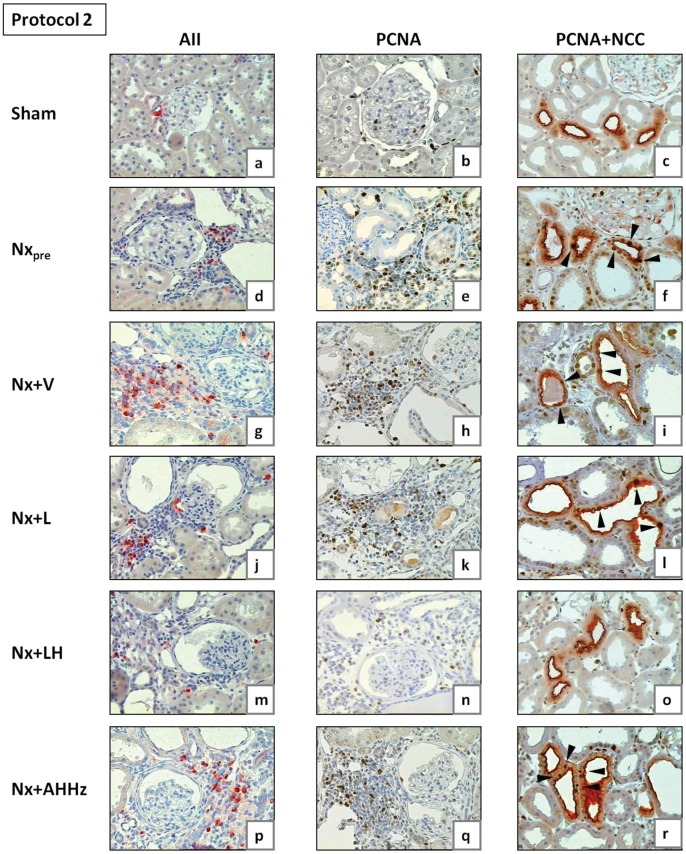
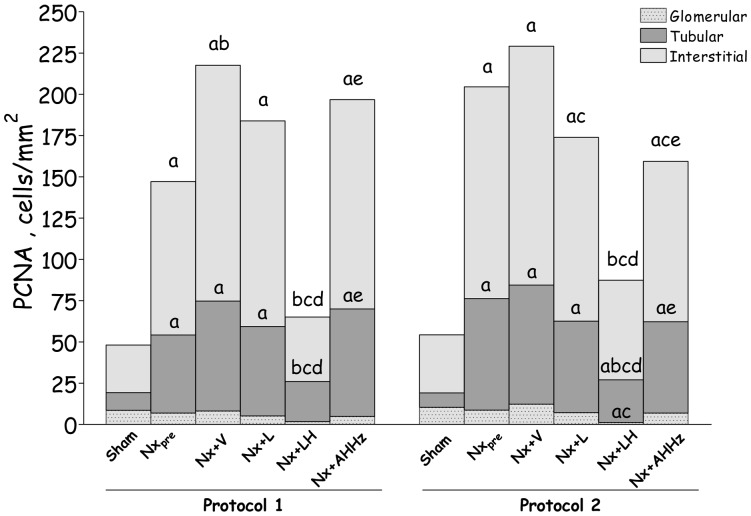
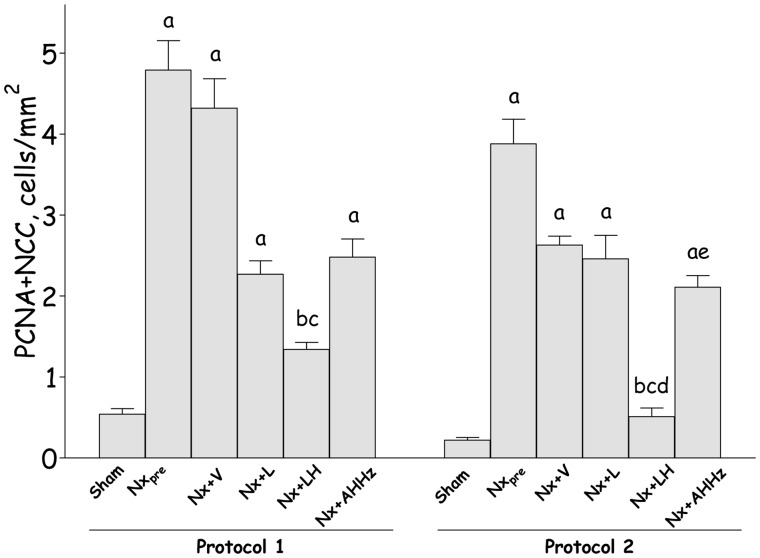
Treatments that effectively prevent chronic kidney disease (CKD) when initiated early often yield disappointing results when started at more advanced phases. We examined the long-term evolution of renal injury in the 5/6 nephrectomy model (Nx) and the effect of an association between an AT-1 receptor blocker, losartan (L), and hydrochlorothiazide (H), shown previously to be effective when started one month after Nx. Adult male Munich-Wistar rats underwent Nx, being divided into four groups: Nx+V, no treatment; Nx+L, receiving L monotherapy; Nx+LH, receiving the L+H association (LH), and Nx+AHHz, treated with the calcium channel blocker, amlodipine, the vascular relaxant, hydralazine, and H. This latter group served to assess the effect of lowering blood pressure (BP). Rats undergoing sham nephrectomy (S) were also studied. In a first protocol, treatments were initiated 60 days after Nx, when CKD is at a relatively early stage. In a second protocol, treatments were started 120 days after Nx, when glomerulosclerosis and interstitial fibrosis are already advanced. In both protocols, L treatment promoted only partial renoprotection, whereas LH brought BP, albuminuria, tubulointerstitial cell proliferation and plasma aldosterone below pretreatment levels, and completely detained progression of renal injury. Despite normalizing BP, the AHHz association failed to prevent renal damage, indicating that the renoprotective effect of LH was not due to a systemic hemodynamic action. These findings are inconsistent with the contention that thiazides are innocuous in advanced CKD. In Nx, LH promotes effective renoprotection even at advanced stages by mechanisms that may involve anti-inflammatory and intrarenal hemodynamic effects, but seem not to require BP normalization.
Conflict of interest statement
Figures
References
-
- Fujihara CK, Noronha IL, Malheiros, Antunes GR, de Oliveira IB, et al. (2000) Combined mycophenolate mofetil and losartan therapy arrests established injury in the remnant kidney. J Am Soc Nephrol 11: 283–290. - PubMed
-
- Fujihara CK, Velho M, Malheiros DM, Zatz R (2005) An extremely high dose of losartan affords superior renoprotection in the remnant model. Kidney Int 67: 1913–1924. - PubMed
-
- Goncalves AR, Fujihara CK, Mattar AL, Malheiros DM, Noronha Ide L, et al. (2004) Renal expression of COX-2, ANG II, and AT1 receptor in remnant kidney: strong renoprotection by therapy with losartan and a nonsteroidal anti-inflammatory. Am J Physiol Renal Physiol 286: F945–954. - PubMed
-
- Fujihara CK, Malheiros DM, Zatz R, Noronha IL (1998) Mycophenolate mofetil attenuates renal injury in the rat remnant kidney. Kidney Int 54: 1510–1519. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
