

Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: a 10-year, single-center experience
- PMID: 23432974
- PMCID: PMC3664270
- DOI: 10.1111/tid.12060
Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: a 10-year, single-center experience
Abstract
Background: The epidemiology of invasive mold infections (IMI) in transplant recipients differs based on geography, hosts, preventative strategies, and methods of diagnosis.
Methods: We conducted a retrospective observational study to evaluate the epidemiology of proven and probable IMI, using prior definitions, among all adult hematopoietic stem cell transplant (HSCT) and solid organ transplant (SOT) recipients in the era of "classic" culture-based diagnostics (2000-2009). Epidemiology was evaluated before and after an initiative was begun to increase bronchoscopy in HSCT recipients after 2005.
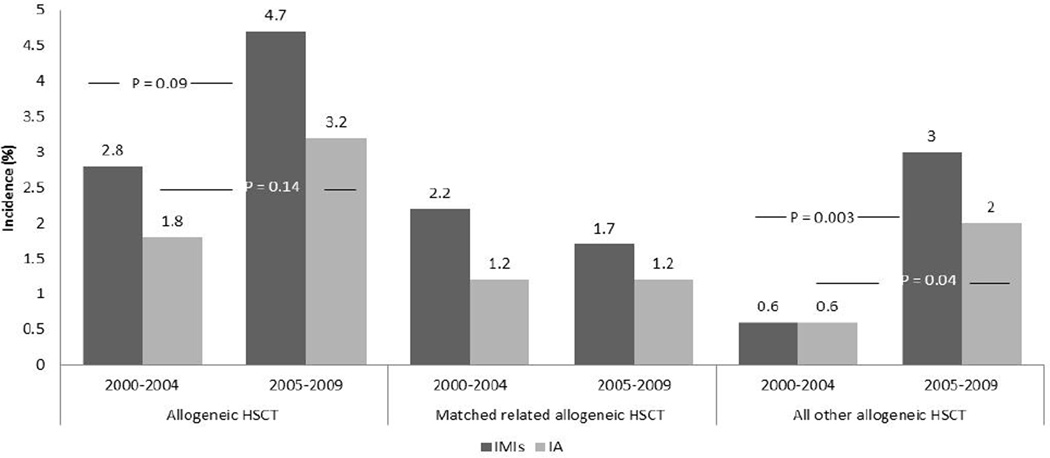
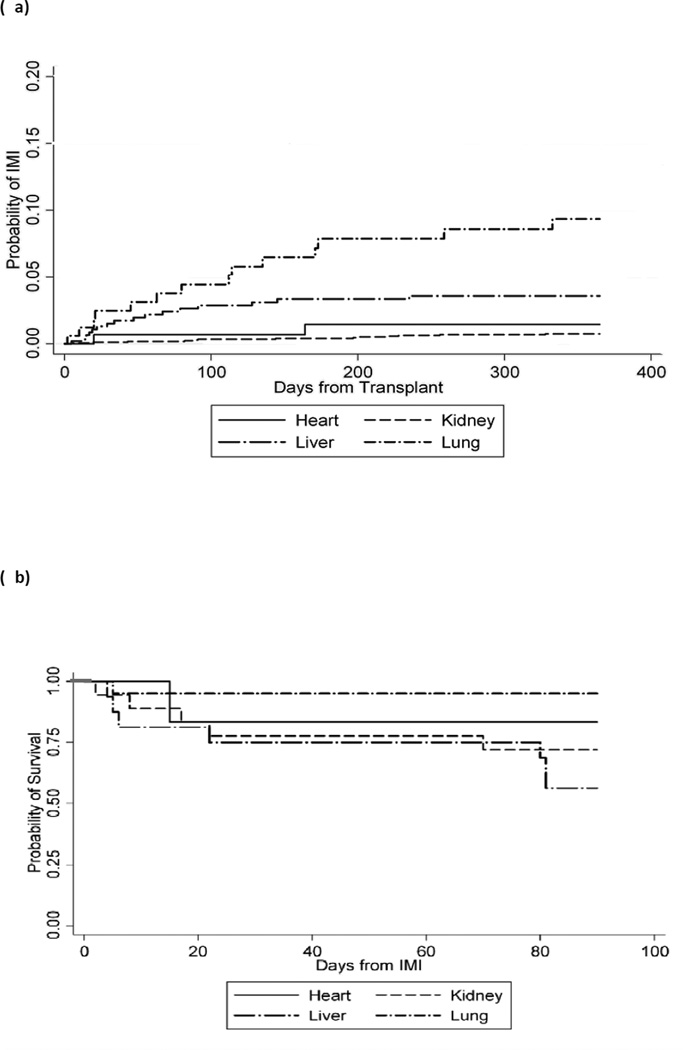
Results: In total, 106 patients with one IMI were identified. Invasive aspergillosis (IA) was the most common IMI (69; 65.1%), followed by mucormycosis (9; 8.5%). The overall rate of IMI (and IA) was 3.5% (2.5%) in allogeneic HSCT recipients. The overall incidence for IMI among lung, kidney, liver, and heart transplant recipients was 49, 2, 11, and 10 per 1000 person-years, respectively. The observed rate of IMI among human leukocyte antigen-matched unrelated and haploidentical HSCT recipients increased from 0.6% annually to 3.0% after bronchoscopy initiation (P < 0.05). The 12-week mortality among allogeneic HSCT, liver, kidney, heart, and lung recipients with IMI was 52.4%, 47.1%, 27.8%, 16.7%, and 9.5%, respectively. Among allogeneic HSCT (odds ratio [OR]: 0.07, P = 0.007) and SOT (OR: 0.22, P = 0.05) recipients with IA, normal platelet count was associated with improved survival. Male gender (OR: 14.4, P = 0.007) and elevated bilirubin (OR: 5.7, P = 0.04) were significant predictors of mortality for allogeneic HSCT and SOT recipients with IA, respectively.
Conclusions: During the era of culture-based diagnostics, observed rates of IMI were low among all transplants except lung transplant recipients, with relatively higher mortality rates. Diagnostic aggressiveness and host variables impact the reported incidence and outcome of IMI and likely account for institutional variability in multicenter studies. Definitions to standardize diagnoses among SOT recipients are needed.
© 2013 John Wiley & Sons A/S.
Conflict of interest statement
Figures
References
-
- [last accessed June 30, 2011]; www.ustransplant.org.
-
- Marr KA, Carter RA, Boeckh M, Martin P, Corey L. Invasive aspergillosis in allogeneic stem cell transplant recipients: Changes in epidemiology and risk factors. Blood. 2002;100(13):4358–4366. - PubMed
-
- Kontoyiannis DP, Wessel VC, Bodey GP, Rolston KV. Zygomycosis in the 1990s in a tertiary-care cancer center. Clin Infect Dis. 2000;30(6):851–856. - PubMed
-
- Marr KA, Carter RA, Crippa F, Wald A, Corey L. Epidemiology and outcome of mould infections in hematopoietic stem cell transplant recipients. Clin Infect Dis. 2002;34(7):909–917. - PubMed
-
- Cordonnier C, Ribaud P, Herbrecht R, et al. Prognostic factors for death due to invasive aspergillosis after hematopoietic stem cell transplantation: a 1-year retrospective study of consecutive patients at French transplantation centers. Clin Infect Dis. 2006;42(7):955–963. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
