

Prevalence of diabetic nephropathy complicating non-diabetic renal disease among Chinese patients with type 2 diabetes mellitus
- PMID: 23432977
- PMCID: PMC3598553
- DOI: 10.1186/2047-783X-18-4
Prevalence of diabetic nephropathy complicating non-diabetic renal disease among Chinese patients with type 2 diabetes mellitus
Abstract
Background: The incidence of diabetes mellitus (DM) and diabetic nephropathy (DN) have risen rapidly in the past few decades and have become an economic burden to the healthcare system in China. DN is a major complication of DM and is a leading cause of end-stage renal disease (ESRD). The occurrence of non-diabetic renal disease (NDRD) in diabetic patients has been increasingly recognized in recent years. It is generally believed that it is difficult to reverse DN, whereas some cases of NDRD are readily treatable and remittable. However, DN is known to co-exist with NDRD in a poorly defined population of patients with type 2 diabetes mellitus (T2DM). This study estimated the prevalence of co-existing DN and NDRD in Chinese patients.
Methods: Data were retrospectively analyzed from 244 patients with T2DM who had undergone a renal biopsy between January 2003 and December 2011 at the Nephrology Department, China-Japan Friendship Hospital, China. Male patients numbered 151 (61.9%) of the study population. The biopsies were performed because urinary abnormalities or renal function were atypical of a diagnosis of DN. Biopsy samples were examined using light, immunofluorescence (IF) and electron microscopy (EM). Clinical parameters were recorded for each patient at the time of biopsy.
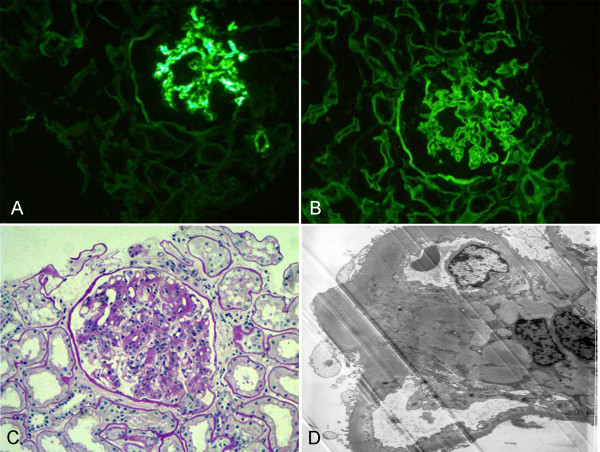
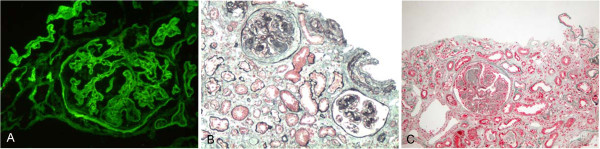
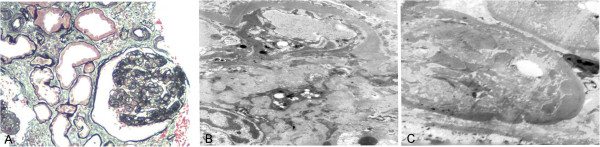
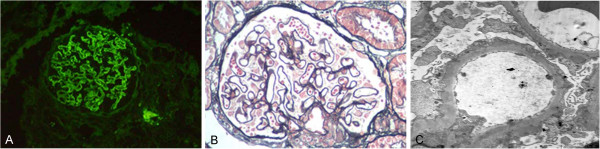
Results: Nineteen of 244 diabetic patients (7.8%) had co-existing DN and NDRD. These patients showed clinical features and pathologic characteristics of DN, including a high prevalence of diabetic retinopathy (89.5%), a long duration of diabetes, increased thickness of the glomerular basement membrane (GBM) and mesangial expansion. However, they also presented with clinical findings which were inconsistent with DN, such as hematuria, rapidly progressive renal failure and marked proteinuria. Immunoglobulin A (IgA) nephropathy was apparent in 10 out of the 19 patients (52.6%), tubulointerstitial lesions were found in four patients (21.1%), membrano-proliferative glomerulonephritis (MPGN) in three patients (15.8%) and membranous nephropathy (MN) in two patients (10.5%).
Conclusion: Retrospective analysis of biopsy data suggests that approximately 8% of Chinese patients with T2DM may have co-existing DN and NDRD. The most common histological diagnosis in our small series was IgA nephropathy.
Figures
References
-
- Suzuki Y, Ueno M, Hayashi H, Nishi S, Satou H, Karasawa R, Inn H, Suzuki S, Maruyama Y, Arakawa M. A light microscopic study of glomerulosclerosis in Japanese patients with noninsulin-dependent diabetes mellitus: the relationship between clinical and histological features. Clin Nephrol. 1994;42(3):155–162. - PubMed
-
- Ruggenenti P, Gambara V, Perna A, Bertani T, Remuzzi G. The nephropathy of non-insulin-dependent diabetes: predictors of outcome relative to diverse patterns of renal injury. J Am Soc Nephrol. 1998;9(12):2336–2343. - PubMed
-
- Gambara V, Mecca G, Remuzzi G, Bertani T. Heterogeneous nature of renal lesions in type II diabetes. J Am Soc Nephrol. 1993;3(8):1458–1466. - PubMed
-
- Spijkerman AM, Dekker JM, Nijpels G, Adriaanse MC, Kostense PJ, Ruwaard D, Stehouwer CD, Bouter LM, Heine RJ. Microvascular complications at time of diagnosis of type 2 diabetes are similar among diabetic patients detected by targeted screening and patients newly diagnosed in general practice: the hoorn screening study. Diabetes Care. 2003;26(9):2604–2608. doi: 10.2337/diacare.26.9.2604. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
