

Amelioration of hypoglycemia via somatostatin receptor type 2 antagonism in recurrently hypoglycemic diabetic rats
- PMID: 23434929
- PMCID: PMC3712070
- DOI: 10.2337/db12-1523
Amelioration of hypoglycemia via somatostatin receptor type 2 antagonism in recurrently hypoglycemic diabetic rats
Abstract
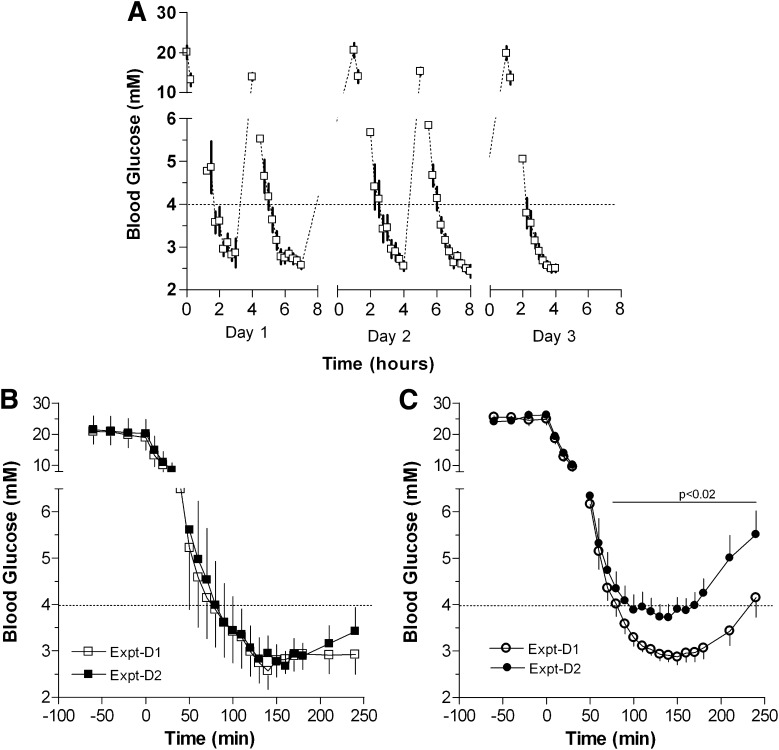
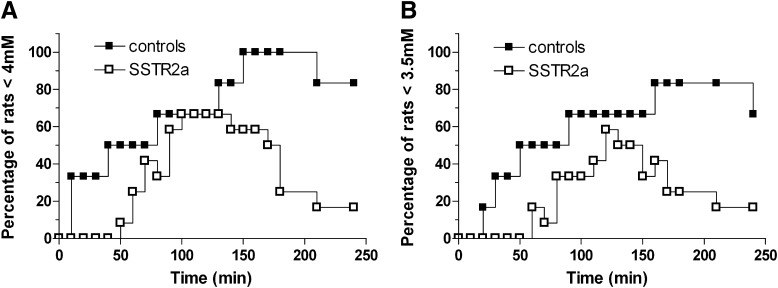
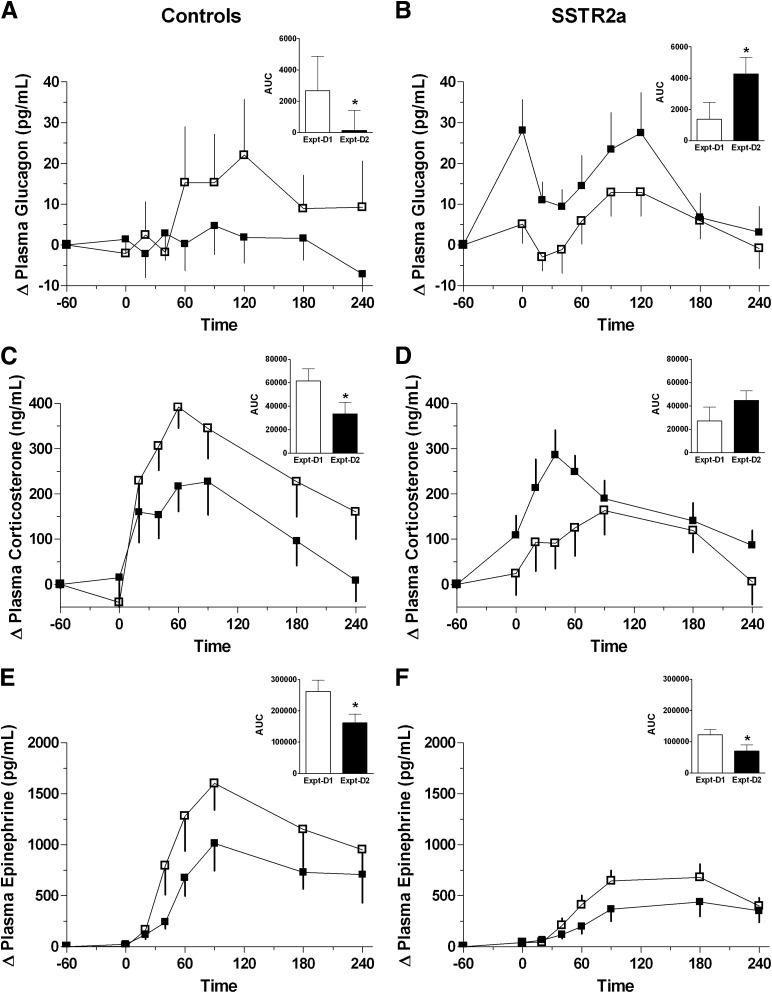
Selective antagonism of somatostatin receptor type 2 (SSTR2) normalizes glucagon and corticosterone responses to hypoglycemic clamp in diabetic rats. The purpose of this study was to determine whether SSTR2 antagonism (SSTR2a) ameliorates hypoglycemia in response to overinsulinization in diabetic rats previously exposed to recurrent hypoglycemia. Streptozotocin diabetic rats (n = 19), previously subjected to five hypoglycemia events over 3 days, received an insulin bolus (10 units/kg i.v.) plus insulin infusion (50 mU/kg/min i.v.) until hypoglycemia ensued (≤3.9 mmol/L) (experimental day 1 [Expt-D1]). The next day (Expt-D2), rats were allocated to receive either placebo treatment (n = 7) or SSTR2a infusion (3,000 nmol/kg/min i.v., n = 12) 60 min prior to the same insulin regimen. On Expt-D1, all rats developed hypoglycemia by ∼90 min, while on Expt-D2, hypoglycemia was attenuated with SSTR2a treatment (nadir = 3.7 ± 0.3 vs. 2.7 ± 0.3 mmol/L in SSTR2a and controls, P < 0.01). Glucagon response to hypoglycemia on Expt-D2 deteriorated by 20-fold in the placebo group (P < 0.001) but improved in the SSTR2a group (threefold increase in area under the curve [AUC], P < 0.001). Corticosterone response deteriorated in the placebo-treated rats on Expt-D2 but increased twofold in the SSTR2a group. Catecholamine responses were not affected by SSTR2a. Thus, SSTR2 antagonism after recurrent hypoglycemia improves the glucagon and corticosterone responses and largely ameliorates insulin-induced hypoglycemia in diabetic rats.
Figures
References
-
- Cryer PE. Hypoglycemia: still the limiting factor in the glycemic management of diabetes. Endocr Pract 2008;14:750–756 - PubMed
-
- Workgroup on Hypoglycemia, American Diabetes Association Defining and reporting hypoglycemia in diabetes: a report from the American Diabetes Association Workgroup on Hypoglycemia. Diabetes Care 2005;28:1245–1249 - PubMed
-
- Amiel SA. Cognitive function testing in studies of acute hypoglycaemia: rights and wrongs? Diabetologia 1998;41:713–719 - PubMed
-
- Realsen JM, Chase HP. Recent advances in the prevention of hypoglycemia in type 1 diabetes. Diabetes Technol Ther 2011;13:1177–1186 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
