

Chiari malformation type I: a case-control association study of 58 developmental genes
- PMID: 23437350
- PMCID: PMC3578784
- DOI: 10.1371/journal.pone.0057241
Chiari malformation type I: a case-control association study of 58 developmental genes
Abstract
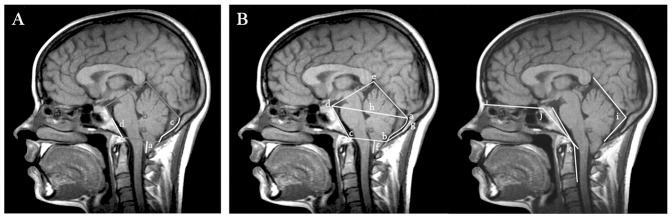
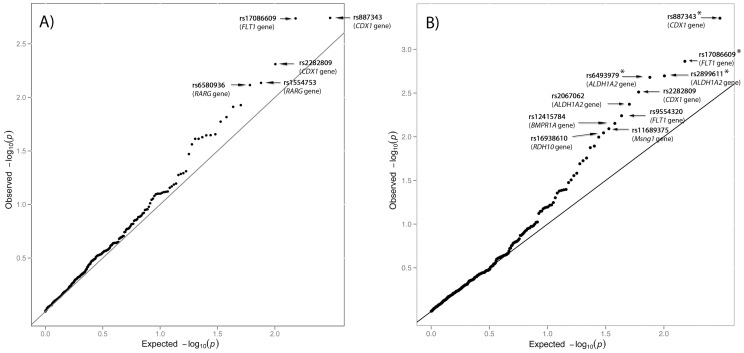
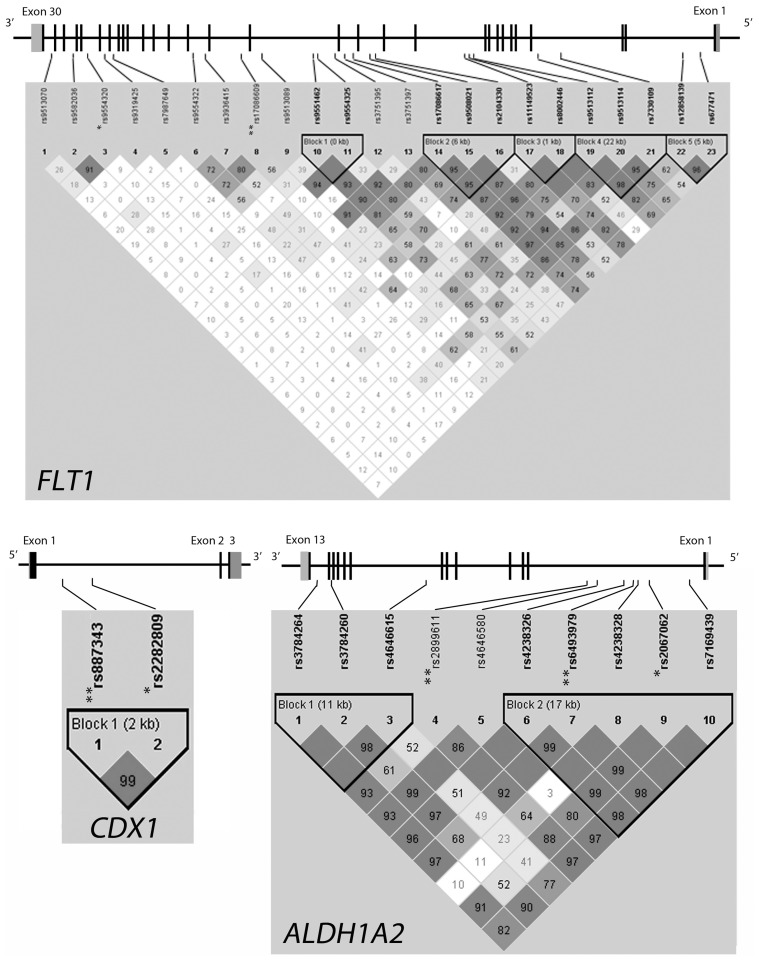
Chiari malformation type I (CMI) is a disorder characterized by hindbrain overcrowding into an underdeveloped posterior cranial fossa (PCF), often causing progressive neurological symptoms. The etiology of CMI remains unclear and is most likely multifactorial. A putative genetic contribution to CMI is suggested by familial aggregation and twin studies. Experimental models and human morphometric studies have suggested an underlying paraxial mesoderm insufficiency. We performed a case-control association study of 303 tag single nucleotide polymorphisms (SNP) across 58 candidate genes involved in early paraxial mesoderm development in a sample of 415 CMI patients and 524 sex-matched controls. A subgroup of patients diagnosed with classical, small-PCF CMI by means of MRI-based PCF morphometry (n = 186), underwent additional analysis. The genes selected are involved in signalling gradients occurring during segmental patterning of the occipital somites (FGF8, Wnt, and retinoic acid pathways and from bone morphogenetic proteins or BMP, Notch, Cdx and Hox pathways) or in placental angiogenesis, sclerotome development or CMI-associated syndromes. Single-marker analysis identified nominal associations with 18 SNPs in 14 genes (CDX1, FLT1, RARG, NKD2, MSGN1, RBPJ1, FGFR1, RDH10, NOG, RARA, LFNG, KDR, ALDH1A2, BMPR1A) considering the whole CMI sample. None of these overcame corrections for multiple comparisons, in contrast with four SNPs in CDX1, FLT1 and ALDH1A2 in the classical CMI group. Multiple marker analysis identified a risk haplotype for classical CMI in ALDH1A2 and CDX1. Furthermore, we analyzed the possible contributions of the most significantly associated SNPs to different PCF morphometric traits. These findings suggest that common variants in genes involved in somitogenesis and fetal vascular development may confer susceptibility to CMI.
Conflict of interest statement
Figures
References
-
- Chiari H (1987) Concerning alterations in the cerebellum resulting from cerebral hydrocephalus. 1891. Pediatr Neurosci 13: 3–8. - PubMed
-
- Milhorat TH, Chou MW, Trinidad EM, Kula RW, Mandell M, et al. (1999) Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients. Neurosurgery 44: 1005–1017. - PubMed
-
- Tubbs RS, Beckman J, Naftel RP, Chern JJ, Wellons JC 3rd, et al. (2011) Institutional experience with 500 cases of surgically treated pediatric Chiari malformation Type I. J Neurosurg Pediatr 7: 248–256. - PubMed
-
- Greenlee JD, Donovan KA, Hasan DM, Menezes AH (2002) Chiari I malformation in the very young child: the spectrum of presentations and experience in 31 children under age 6 years. Pediatrics 110: 1212–1219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
