

Dietary acid load: a novel nutritional target in chronic kidney disease?
- PMID: 23439373
- PMCID: PMC3604792
- DOI: 10.1053/j.ackd.2012.11.001
Dietary acid load: a novel nutritional target in chronic kidney disease?
Abstract
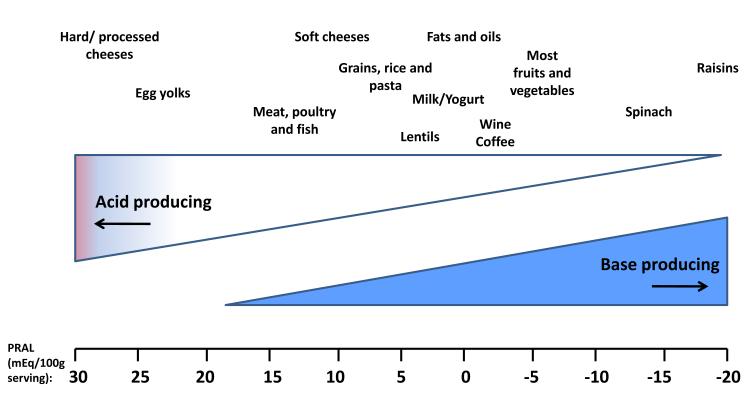
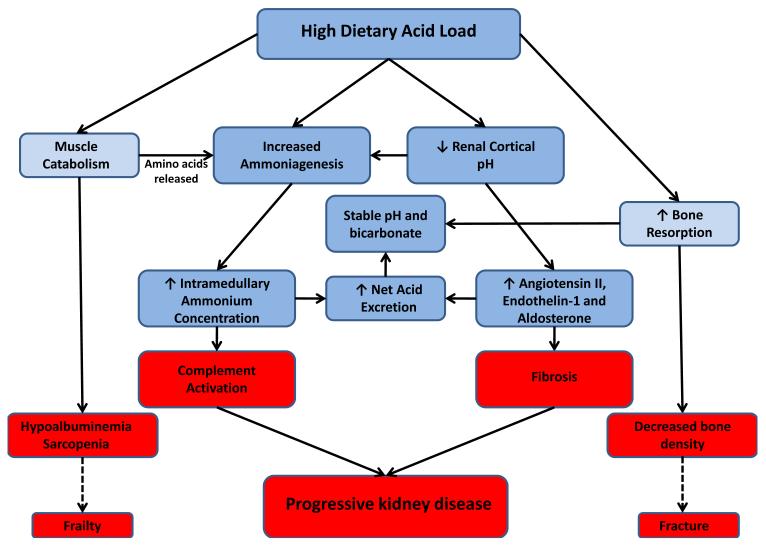
Nonvolatile acid is produced from the metabolism of organic sulfur in dietary protein and the production of organic anions during the combustion of neutral foods. Organic anion salts that are found primarily in plant foods are directly absorbed in the gastrointestinal tract and yield bicarbonate. The difference between endogenously produced nonvolatile acid and absorbed alkali precursors yields the dietary acid load, technically known as the net endogenous acid production, and must be excreted by the kidney to maintain acid-base balance. Although typically 1 mEq/kg/day, dietary acid load is lower with greater intake of fruits and vegetables. In the setting of CKD, a high dietary acid load invokes adaptive mechanisms to increase acid excretion despite reduced nephron number, such as increased per nephron ammoniagenesis and augmented distal acid excretion mediated by the renin-angiotensin system and endothelin-1. These adaptations may promote kidney injury. Additionally, high dietary acid loads produce low-grade, subclinical acidosis that may result in bone and muscle loss. Early studies suggest that lowering the dietary acid load can improve subclinical acidosis, preserve bone and muscle, and slow the decline of glomerular filtration rate in animal models and humans. Studies focusing on hard clinical outcomes are needed.
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Gonick HC, Goldberg G, Mulcare D. Reexamination of the acid-ash content of several diets. Am J Clin Nutr. 1968;21(9):898–903. - PubMed
-
- Sebastian A, Frassetto LA, Sellmeyer DE, Merriam RL, Morris RC., Jr. Estimation of the net acid load of the diet of ancestral preagricultural Homo sapiens and their hominid ancestors. Am J Clin Nutr. 2002;76(6):1308–1316. - PubMed
-
- Strohle A, Hahn A, Sebastian A. Estimation of the diet-dependent net acid load in 229 worldwide historically studied hunter-gatherer societies. Am J Clin Nutr. 2010;91(2):406–412. - PubMed
-
- Remer T, Manz F. Paleolithic diet, sweet potato eaters, and potential renal acid load. Am J Clin Nutr. 2003;78(4):802–803. - PubMed
-
- Cordain L, Eaton SB, Sebastian A, et al. Origins and evolution of the Western diet: health implications for the 21st century. Am J Clin Nutr. 2005;81(2):341–354. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
